Glaucoma: Evolving
Winter 2024
by Liz Hillman
Editorial Co-Director
In August 2024, Lee et al. published a paper that looked at nearly 200,000 initial glaucoma evaluations, finding that 20.4% and 29.5% had a gonioscopy performed on the day of diagnosis or within 6 months of their evaluation, respectively.1 Statistics like this might prompt questions like, “Is gonioscopy dead?” While glaucoma specialists who spoke with EyeWorld said gonioscopy remains a vital and valuable tool in the clinic, newer imaging systems can help visualize the angle as well, overcoming some limitations of gonioscopy and becoming a complementary technology.
“Office-based gonioscopy is alive and well. It forms an integral part of an eye exam … but [is] unfortunately underutilized in clinical practice,” said Shakeel Shareef, MD.
Benjamin Y. Xu, MD, PhD, said he could see how someone who performs gonioscopy regularly, experiencing its limitations frequently, might ask whether gonioscopy is dead or still necessary. He assures those in the field that it still has a place.
Source: Shakeel Shareef, MD
Why office-based gonioscopy remains important
Dr. Xu said gonioscopy remains important for patients having glaucoma evaluations. “The management of open angle glaucoma and angle closure glaucoma differ, so to misclassify a patient means you may not be offering the optimal or ideal treatments,” he said.
In the Lee et al. study, Dr. Xu, who was the corresponding author, said patients with an open angle diagnosis were 10 times less likely to have a gonioscopy compared to angle closure glaucoma. If patients are not receiving gonioscopy, they’re less likely to be diagnosed with angle closure. “Angle closure glaucoma is a very treatable and preventable form of glaucoma early on. You can provide laser and surgery and effectively eliminate the risk of glaucoma, whereas if you presume the patient has open angle glaucoma and treat with eye drops alone, the angle closure can worsen and become difficult to control,” Dr. Xu said. “My general advice is to still perform gonioscopy in all patients receiving glaucoma evaluations because it provides valuable information to guide management.”
He also pointed out that gonioscopy can reveal other abnormalities in the angle, such as neovascularization and iris or ciliary body tumors. “These are devastating to miss early on. In the absence of a more convenient assessment like OCT … we should still continue to perform gonioscopy so we can provide our patients with the standard of care,” Dr. Xu said.
Dr. Shareef listed the different purposes gonioscopy still provides. It 1) differentiates whether the angle is anatomically open or closed; 2) assesses for neovascularization of the angle in patients with diabetic retinopathy; 3) aids in surgical planning of angle-based surgeries; 4) assesses for angle recession in those who have sustained ocular trauma clinically observed as a widening of the ciliary body band; 5) monitors glaucoma suspects and glaucoma patients; 6) evaluates the outflow pathway in high hyperopes who are at risk for acute angle closure; and 7) facilitates laser trabeculoplasty for the ophthalmologist to aim the laser beam and deliver targeted energy to help lower the eye pressure in patients with open angle glaucoma.
Source: Shakeel Shareef, MD
Limitations of office-based gonioscopy
Dr. Xu said the most inconvenient aspect of gonioscopy is it requires putting a contact lens on the patient’s eye typically prior to dilation. “This can be uncomfortable for the patient. It can be time consuming. It can be disruptive to clinical workflows,” he said. “As a clinical assessment, it is not very convenient to perform gonioscopy.”
Another limitation is that there is a high degree of variability between clinicians. “It’s qualitative and not terribly reproducible, so there is also that inherent limitation of the technique,” Dr. Xu said.
Regarding the Lee et al. study, of which Dr. Xu was the corresponding author, he said he and the co-authors were surprised at how few gonioscopies were performed. “Perhaps it speaks to the need for new technology, something that’s more convenient,” he said.
Modern angle imaging
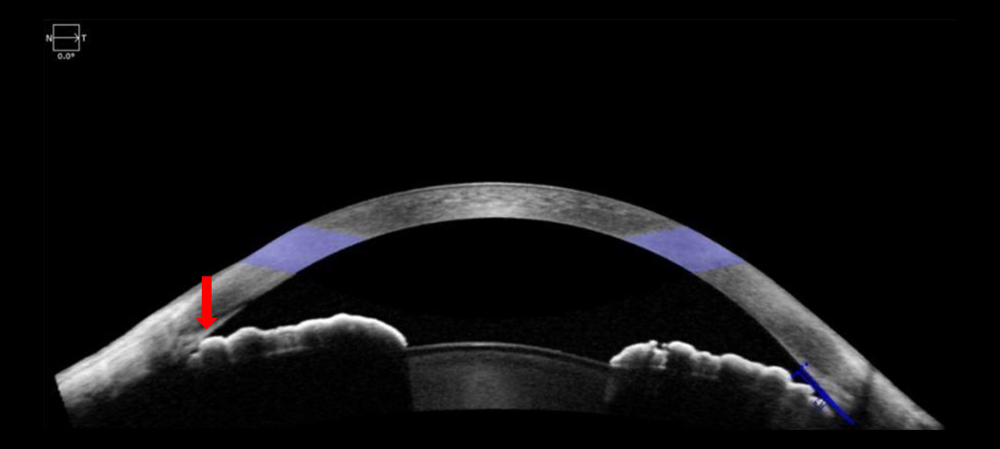
In lieu of or in conjunction with manual gonioscopy, Dr. Shareef said imaging technologies like anterior segment OCT (AS-OCT) and/or ultrasound biomicroscopy (UBM) can play an important role.
He offered this example: “If an asymptomatic patient has anatomically narrow or closed angles determined during an eye exam, the imaging obtained would enable the physician to educate and counsel the patient of their condition, including intervention, as it would be difficult to explain to the patient otherwise. The image demonstrating angle closure would enable a provider to offer the patient options including 1) observation if asymptomatic; 2) laser iridotomy to open the drain as a preventative measure or if symptoms warrant the drain to be opened; 3) if appropriate, the need to perform cataract surgery to anatomically open the drain. This could also be a discussion in the setting of a patent iridotomy, yet the drain remains closed, and the patient is symptomatic with elevated eye pressure that needs to be lowered.”
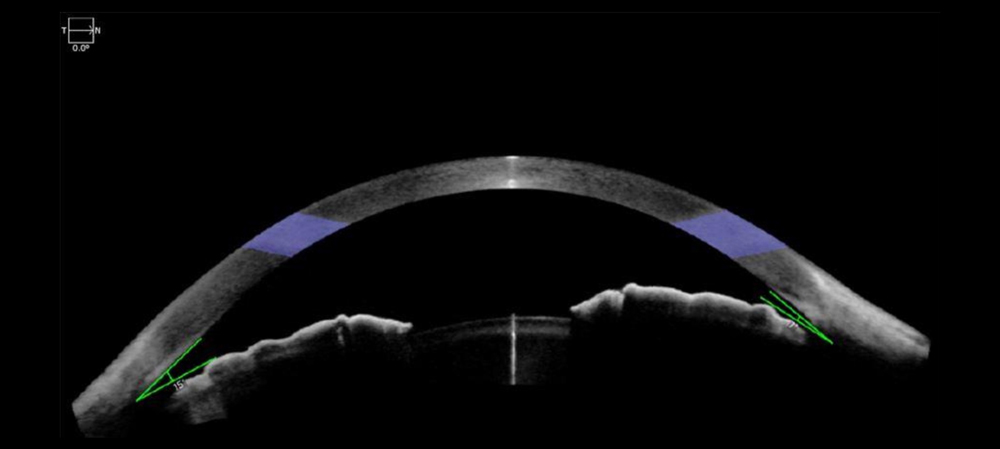
From a diagnostic standpoint, Dr. Shareef said imaging technologies can be helpful for patients who cannot have office-based gonioscopy, such as those who have a shallow or hypotonus eye. Imaging can help identify the location and size of cyclodialysis cleft for surgical planning, for example, or angle closure in the setting of a patent iridotomy in the presence of plateau iris syndrome. “[Imaging] would enable the physician to counsel the patient to consider argon laser iridoplasty to further open the angle to enhance outflow and lower the eye pressure,” Dr. Shareef said.
Dr. Xu said anterior segment OCT for glaucoma is an active area of research.
“One challenge to performing gonioscopy is that it’s qualitative. We describe the structures we can see but we can’t take a precise measurement. It becomes hard to track conditions like angle narrowing or angle closure over time,” he said. “OCT has been around for several decades, and it’s widely used in the posterior segment for measuring anatomical structures like the thickness of the retina. We and other research groups have been adapting OCT for the anterior segment as a means of more precisely quantifying the anatomical configurations of our patients. I think that is a unique strength of OCT, which nicely complements a primary weakness of gonioscopy. In addition, OCT is fast; it doesn’t take a trained clinician to perform; it’s non-contact so it’s comfortable for patients. Analysis of OCT images can also be automated using other technologies, such as artificial intelligence. In these ways, OCT may fill a clinical need for a more convenient and reproducible method to assess the angle.”
Some knowledge from the research being produced with AS-OCT for angle imaging is being transferred to the clinic already. Dr. Xu said he and colleagues compared AS-OCT and gonioscopy for predicting patients with mild angle closure who would go on to develop more severe angle closure.2 They found patients with narrow angles on AS-OCT had a higher risk of progression, whereas gonioscopy was not as predictive. He added they have yet to identify specific cutoffs at which a patient should be considered higher risk and receive treatment, but this research is underway.
A couple of limitations for anterior segment OCT are that it’s expensive and bulky, compared to a gonio lens, which is cheaper and portable.
At this point, UBM of the angle is feasible but has some limitations, according to Dr. Xu. Not only does it require a trained technician to perform, but he said there is generally no way to locate the previous location of imaging (no clear landmarks), making repeatability with measurements difficult.
“It’s hard to know exactly where on the eye you’re imaging. From a reproducibility standpoint, if you image a patient and re-image 6 months later, you might not be in the same location and therefore you might get different measurements,” he said, adding that some companies, like ArcScan, are working on overcoming this limitation.
“It’s not as convenient or as reproducible as AS-OCT,” Dr. Xu continued of UBM. “However, it allows you to look behind the iris, which AS-OCT does not. If you have a ciliary body tumor or a cause of angle closure that originates behind the iris, you can’t see that with AS-OCT.”
As of right now, Dr. Xu said, “we’re primarily trying to implement OCT as a complement to gonioscopy to make clinicians’ lives a bit easier and angle evaluations more precise.”
In the meantime, Dr. Xu and Dr. Shareef advocate for regular office-based gonioscopy on glaucoma patients.
“Imaging typically provides a 2-D view of a representative angle with multiple measurements. Even in those technologies that offer 3-D viewing, there are certain deficiencies inherent with imaging wherein manual gonioscopy provides superior clinical information that imaging cannot,” Dr. Shareef said, including identifying subtle neovascularization of the angle in patients with retinal ischemia, reliable identification of Schwabe’s line and the trabecular meshwork to determine the angle’s status, differentiating between appositional angle closure vs. synechial angle closure, and confirming proper anatomic placement of microstents in Schlemm’s canal postoperatively.
ARTICLE SIDEBAR
In the pipeline
Dr. Shareef said the ViaLux Laser System (ViaLase) combines femtosecond laser with gonioscopic imaging for non-invasive trabeculotomy procedures. “A high-resolution video of the iridocorneal angle allows the surgeon to inspect the angle and to select the desired area of treatment to deliver the laser with minimal collateral damage to adjacent tissue,” he said.
About the physicians
Shakeel Shareef, MD
Director, The Center for Glaucoma & Cataract Care
Chief of the Ophthalmology Section, Department of Surgery
HCA Reston Hospital Center
Reston, Virginia
Benjamin Y. Xu, MD, PhD
Associate Professor of Clinical Ophthalmology
Chief of the Glaucoma Service
Director of Data Science and Artificial Intelligence
USC Roski Eye Institute
Keck School of Medicine
Los Angeles, California
References
- Lee JH, et al. Patterns and disparities in recorded gonioscopy during initial glaucoma evaluations in the United States. Am J Ophthalmol. 2024:264;90–98.
- Xu BY, et al. Ocular biometric risk factors for progression of primary angle closure disease: the Zhongshan Angle Closure Prevention Trial. Ophthalmology. 2022;129:267–275.
Relevant disclosures
Shareef: None
Xu: ArcScan, Heidelberg Engineering
Contact
Shareef: drshareef@glaucomacc.com
Xu: Benjamin.Xu@med.usc.edu