Cataract: Complicated cases
September 2023
by Liz Hillman
Editorial Co-Director
Precise placement and subsequent stability of a toric IOL are of the utmost importance for success in correcting astigmatism. Capsule tears can threaten both factors. So what do you do when a capsule tear occurs during cataract surgery when you planned to implant a toric IOL?
Amandeep Rai, MD, FRCSC, said recognition is the first step with any case of capsule rent, whether or not a toric IOL is planned.
“Once recognized, the surgeon should try to immediately tamponade the vitreous behind the compromised capsule with a dispersive viscoelastic device. It is incumbent on the surgeon to ensure that the anterior chamber remains formed; sudden shallowing may cause the rent to suddenly enlarge,” Dr. Rai said. “Depending on the stage of the surgery, the surgeon should attempt to keep all lens material anterior to the rent and remove the cataract with altered fluidics. Generous use of viscoelastic can help compartmentalize the lens fragments in the anterior chamber and keep the vitreous posterior.
“A surgeon should alter the fluidics by reducing the flow rate, irrigation pressure, and vacuum,” Dr. Rai continued. “Irrigation and aspiration may be done manually or at low flow settings. Surgeons should ensure that there is no vitreous prolapse, and this may be aided by the use of diluted triamcinolone intracamerally. Any vitreous should be removed using a vitrector, and the surgeon should be vigilant and check for vitreous regularly through the remainder of the case. Suturing the main wound is suggested, as this patient may require a vitrectomy and is also at increased risk of postoperative endophthalmitis. Intracameral antibiotics should also be considered.”
When it comes to IOL selection, Dr. Rai said it depends on capsular support and the type of rent. If it is an anterior capsule (AC) rent, Dr. Rai said that a single-piece IOL can be placed if the surgeon is confident in the long-term axial and rotational stability.
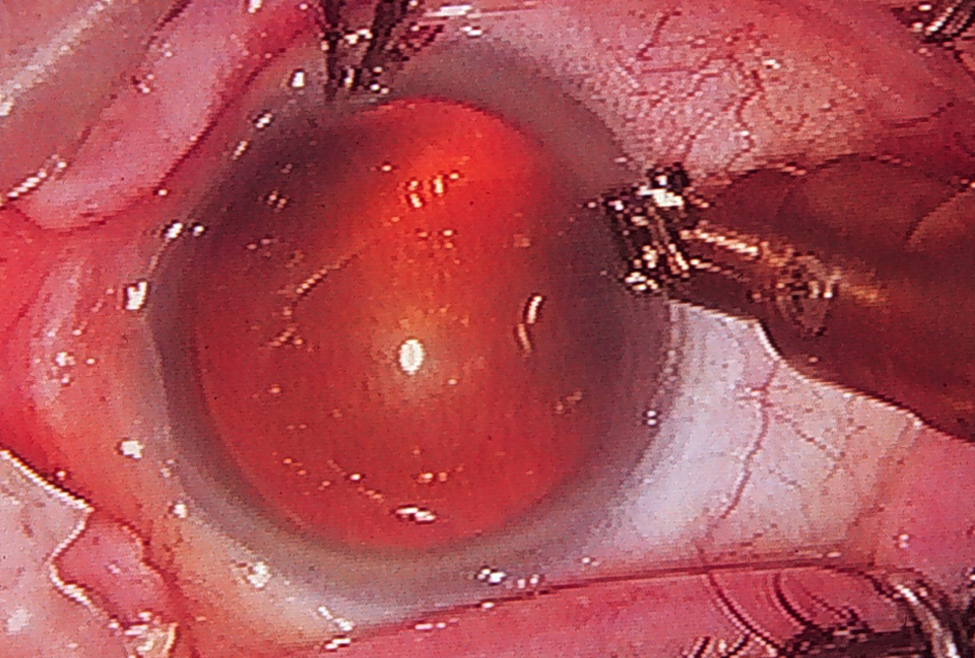
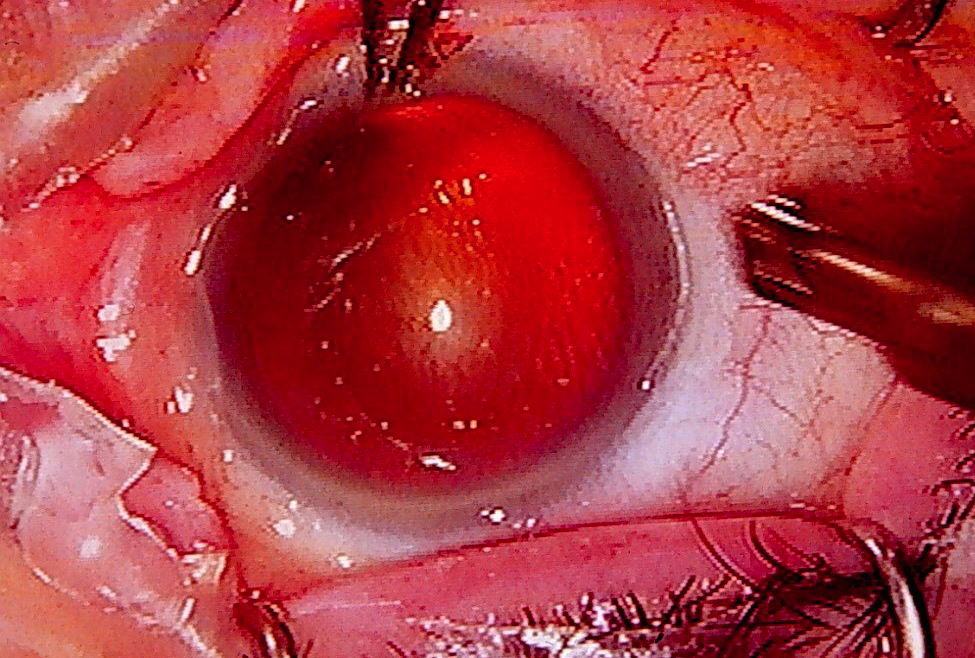
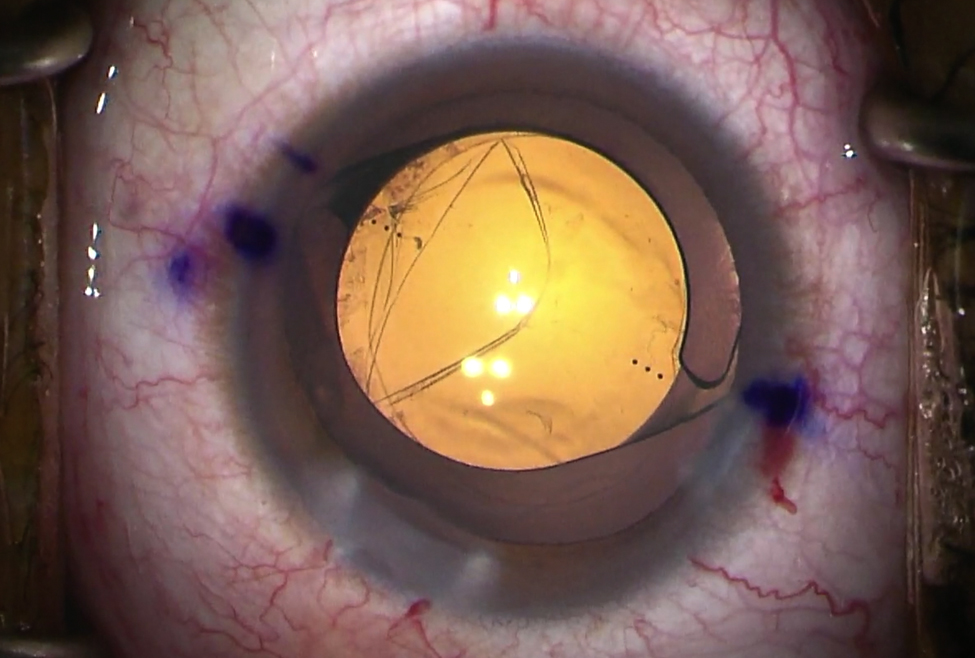
Source (all): Jonathan Rubenstein, MD
“This depends on appropriate placement of the haptics so that a haptic does not tilt forward; if a single haptic is in the bag and the other haptic tilts forward into the sulcus, the patient is at high risk for postoperative uveitis- glaucoma-hyphema (UGH) syndrome,” he said. “The tilt can also induce astigmatism and/or coma. The ideal scenario would be a small AC rent that happens to coincide with the steep axis of corneal astigmatism. This would allow the physician to orient the toric IOL such that the haptic-optic junction is around the area of the rent, and both haptics will be entirely secured under the remaining capsulorhexis edge.”
A single-piece IOL may also be an option in the setting of a posterior capsule rupture (PCR), provided the posterior capsule surface area is large enough to support the IOL long term.
“If the surgeon is able to keep the PCR small and controlled throughout the remainder of the surgery, a single-piece IOL is certainly a plausible outcome; in that scenario, a toric IOL should be considered,” he said. “This is especially true if the PCR can be converted to a posterior continuous curvilinear capsulorhexis. If the PCR is large and the surgeon thinks that the remaining posterior capsule cannot support an IOL, a common IOL placement is in the sulcus (with or without optic capture). In this scenario, the surgeon should not place a single-piece toric IOL in the sulcus due to the increased risk of UGH syndrome. Instead, a three-piece IOL with PMMA haptics should be used. An alternate option for placement of a single-piece IOL in the setting of a PCR is reverse optic capture; a single-piece IOL can be placed with the haptics in the capsular bag and the optic anterior to the capsulorhexis opening. This technique of reverse optic capture would allow a surgeon to still implant a single-piece toric IOL in a compromised capsule.”
If capsular support is entirely insufficient, Dr. Rai also mentioned anterior chamber IOLs, iris-sutured IOLs, scleral-sutured IOLs, and intrascleral haptic fixation as possibilities.
Jonathan Rubenstein, MD, shared his thoughts on what to do when there is a compromised capsule and a toric IOL was planned. If there is a PC tear, he said you need to make sure you can visualize the entire extent of the tear to ensure that it won’t tear out, producing instability. If it’s localized (and ideally round), Dr. Rubenstein said it’s unlikely to tear out, and thus OK to place a toric IOL, provided the zonules are still good.
“During placement, avoid further extension of the posterior capsule, using OVD to protect the capsular bag,” he said.
Dr. Rubenstein said if it’s not advisable to place a toric IOL, you can still address astigmatism in the OR. If you’ve planned for it or have a nomogram and the proper equipment available, you could perform limbal relaxing incisions (LRIs), he said. He added that he doesn’t think many surgeons are comfortable or have the equipment/information available to them in the OR to perform this procedure, if they weren’t already planning for it.
Postop management of astigmatism, if a monofocal IOL was placed due to the compromised capsule, includes glasses, toric contact lenses, or a refractive procedure, such as corneal refractive surgery, LRIs, astigmatic keratectomy, and opposite clear corneal incision. Dr. Rubenstein said these are options for patients who had a three-piece lens in the sulcus or placed with optic capture. He lets these patients stabilize for 3 months post-cataract surgery because “at that point, it’s refractive astigmatism rather than astigmatism based on corneal measurement.”
The physicians also addressed the patient counseling aspect of this complication.
“The discussion,” Dr. Rubenstein said, “is: ‘Our first priority is to get your cataract out safely and completely, which we were able to accomplish. … Second, we want to put a lens implant in your eye that is as close to the correct power and as stable as possible, and we were able to accomplish that. Third is to try to produce the lowest residual refractive error … as possible, and we’re able to correct hopefully the spherical part of your refraction, but you still have astigmatism, which we were not able to correct in surgery, and we will offer you the opportunity to correct that later.’ We’ll say something like, ‘During surgery we assessed that your eye was not stable enough to support the type of lens implant that we originally had planned to correct astigmatism; we thought it was unsafe to use that kind of lens because we couldn’t be assured it would stay in the position that was needed to fully correct your astigmatism, and therefore we put in a lens implant that does not correct astigmatism because it was the most stable lens for your eye. We can always come back later and correct your astigmatism.’”
Dr. Rai also said it’s important to thoroughly discuss this situation with the patient and their family postop, namely because these patients are at increased risk for complications, such as high intraocular pressure in the first few hours postop, endophthalmitis in the days postop, and/or retinal tear/detachment, CME, or pseudophakic bullous keratopathy in the weeks postop.
“They may also need further surgery for retained fragments. As such, patient education is important so they may seek immediate and appropriate care for any postoperative complications. These patients should also be scheduled for close follow-up to monitor for complications and ensure a safe recovery,” Dr. Rai said.
Overall, Dr. Rai said that patients with astigmatism can benefit from a well-placed toric IOL, and even in the setting of some capsular complications, it is still possible, depending on a few factors, to deliver the best possible uncorrected distance visual acuity to patients.
article sidebar
Is there still a place for AK and LRIs?
Dr. Rubenstein said he has taught skills transfer labs for astigmatic keratectomy (AK) and limbal relaxing incisions (LRIs) at major medical meetings for many years, and every year, ahead of the lab, he would think, “This is dying.” However, attendance would prove him wrong. “Every year there is still interest. People think this should still be in surgeons’ toolbox,” he said.
It’s good for very small amounts of astigmatism, Dr. Rubenstein continued, noting that in the U.S., toric IOLs correct 1–1.25 D of astigmatism minimum. LRIs, in contrast, can correct less than that. Another indication, Dr. Rubenstein said, is higher amounts of astigmatism. LRIs can be performed in addition to a toric IOL to improve quality of vision.
“I think there still is a place for this, and based on what happens at our meetings each year, there is still an interest in them,” Dr. Rubenstein said, noting that his program trains residents to perform LRIs and AKs. “It’s part of the surgical armamentarium we should know about.”
About the physicians
Amandeep Rai, MD, FRCSC
Residency Program Director
Department of Ophthalmology and Vision Sciences
University of Toronto
Toronto, Canada
Jonathan Rubenstein, MD
Professor and Chairman
Department of Ophthalmology
Rush University Medical Center
Chicago, Illinois
Relevant disclosures
Rai: Alcon, Bausch Health
Rubenstein: Alcon
Contact
Rai: amandeep.rai@mail.utoronto.ca
Rubenstein: Jonathan_Rubenstein@rush.edu