Cornea
September 2023
by Ellen Stodola
Editorial Co-Director
Losartan is being studied as a potential treatment for corneal fibrosis and scarring. Steven E. Wilson, MD, has been conducting studies on the use of topical losartan in this area.1 He spoke to EyeWorld about the status of those (mostly animal) studies, experience with off-label applications in human patients, and his thoughts about this option becoming more available.
Many compounding pharmacies are now preparing this for use around the U.S., he said, noting that topical losartan was the number one trending medication at compounding pharmacies in April of this year.
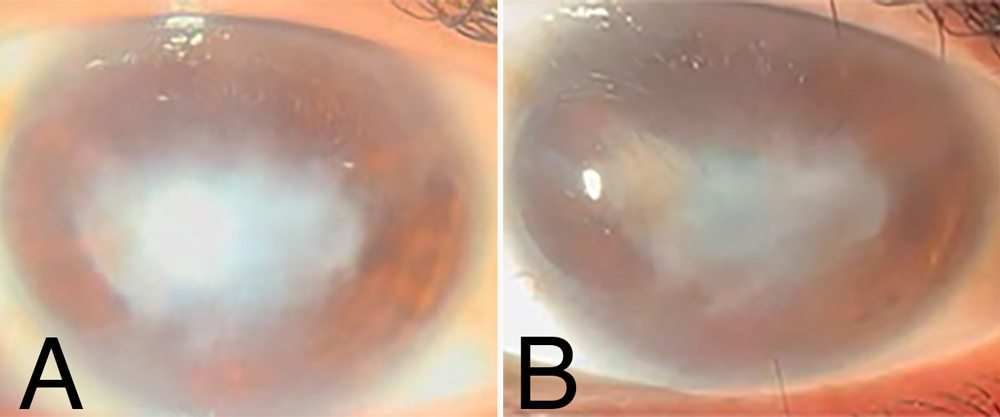
Source: Danyelle Medeiros, MD
Dr. Wilson became interested in researching this and has been funded for more than 30 years by NIH and DOD. “Earlier in my career, every week I read the full issue of Science when it came out,” he said. “In 2011, there was an article published that showed that losartan inhibited fibrosis in the aorta in animal models when given orally.” Years later, Dr. Wilson remembered the article and decided to pursue this area of research with a DOD grant, which looked at whether topical losartan would impact topical scarring fibrosis in the cornea.
He used several models to research this. The first he chose was descemetorhexis2 because it had been recently demonstrated that when you remove Descemet’s membrane and endothelium (about an 8-mm patch) in rabbits, they get severe posterior corneal fibrosis. “The reason that appealed to me as the first place to test it is because the epithelium and basement membrane in those corneas is normal,” he said. “If the losartan could penetrate the intact normal epithelium and intact epithelial basement membrane and still impact the posterior fibrosis, that means it could treat anything in the cornea.”
Most drugs can’t penetrate the intact epithelium and epithelial basement membrane, Dr. Wilson said. For example, in a patient who has fibrosis after PRK, their epithelium heals normally, but a few months later, they develop severe scarring fibrosis of the cornea. Any drug that doesn’t penetrate the epithelium and epithelial basement membrane is not going to be effective. “The study not only showed that losartan was effective against corneal fibrosis but also that it could work in a cornea where the epithelium and epithelial basement membrane are intact.”
Dr. Wilson said there are dozens of companies that have brainstormed ideas for drugs that will impact corneal fibrosis when given topically. Many have reached out for his opinion, and Dr. Wilson said the first question he asks is if it penetrates the epithelium and epithelial basement membrane. The answer is almost always no, but now it’s been proven that losartan does.
“I encourage physicians not to use more than 0.8 mg/mL until animal studies show that higher concentrations are safe and effective. It’s working so well now.”
Steven E. Wilson, MD
Dr. Wilson’s work includes five studies in rabbits, three of which are published, one that is in review, and another that is being prepared for publication. One study was for descemetorhexis, one was for alkali burns,3 and a third was in PRK in rabbits. “One study simulated a blast injury to the cornea, and we used that with an irregular excimer laser ablation that simulates a very rough corneal surface, while the last study investigated the effect of losartan on incisions in rabbit corneas,” he said.
The Cleveland Clinic has submitted a patent covering losartan and all the other drugs in that group, Dr. Wilson said, adding that there are at least eight other angiotensin II receptor blockers.
Losartan was the drug that was initially focused on because it has shown several advantages, with the first being that it’s soluble in basic buffers like balanced salt solution or normal saline. Most other drugs in that group are not soluble in aqueous solutions, so you’d have to use special vehicles. This adds more complexity for formulating it for patients.
Losartan is also one of the most widely used oral drugs in the world, so the safety is assured, he said. It’s now been used topically by hundreds of ophthalmologists throughout the world.
Dr. Wilson has trained a number of Brazilian corneal and refractive surgeons and noted that the first in-human case report using losartan for a refractive surgery complication came from Renato Ambrosio Jr., MD, PhD, who contacted Dr. Wilson about one of his patients who he thought would benefit from this.4 Since this first case, Dr. Wilson said he has heard from many other ophthalmologists with cases where they think losartan could be used.
Dr. Wilson noted that a critical piece is that “you can’t stop after 1 month of treatment and think that the patient failed.” Some patients will start responding by 2 or 3 months. “In the vast majority, especially the more severe scarring fibrosis, it’s going to take 4–6 months before you see that it’s working,” he said. He noted that patients may notice an improvement in vision before physicians see it at the slit lamp. It’s important to get a commitment from the patient to try this option for 6 months before giving up. Dr. Wilson noted that of the few patients who have been using it for almost a year, there have been no reports of toxicity.
However, he cautioned that those interested in exploring this treatment option stick to the recommended and proven dosage of 0.8 mg/mL. While many have asked if it would make sense to increase the dosage for the treatment to work faster, this could cause complications because you start interfering with normal functions that transforming growth factor beta controls in the cornea. “I encourage physicians not to use more than 0.8 mg/mL until animal studies show that higher concentrations are safe and effective. It’s working so well now,” he said.
His research has shown that losartan is soluble up to more than 400 mg/mL in balanced salt solution, but when you get up to this amount, it becomes viscous like hyaluronic acid-containing solutions. “I don’t want physicians applying that to corneas before higher doses have been tried in animals. My biggest concern is that people will start using higher concentrations with no data and end up with complications that have not been reported with the 0.8 mg/mL dosage since transforming growth factor beta also regulates normal cellular functions in corneas,” he said, emphasizing that he has yet to have any reports of complications in patients using it 6 times a day for months.
Dr. Wilson pointed out that animal studies that have been done have so far have been prophylactic. But the human studies are in patients who already have the fibrosis and start treatment. This proves that the treatment could work either way. “It works prophylactically because transforming growth factor beta is required for the precursor cells to develop into myofibroblasts,” he said. “Or it works if the fibrosis is already there because the myofibroblasts that maintain the fibrosis are still dependent on an ongoing adequate supply of transforming growth factor beta signaling. If you cut that off with losartan, you’ll cause those cells to undergo apoptosis, and when that happens, normal keratocytes and corneal fibroblasts can repopulate that area of the cornea and restore the normal transparent arrangement of the stromal tissue.” This will require further research, as Dr. Wilson noted that patients who have been treated so far only had scarring for no more than a year or two. “The question is if it would still work on someone who had a terrible herpes simplex infection 10 years ago and has a scarred cornea,” he said.
Dr. Wilson said the use of losartan could have applications beyond the cornea as well, which makes it an exciting option to keep studying. He noted research being done by Victor Perez, MD, looking at losartan applications on different conjunctival fibrotic diseases, such as Stevens-Johnson syndrome, graft versus host disease, and bullous pemphigoid. None of these have very effective treatment, Dr. Wilson said, and the end pathology is transforming growth factor beta-mediated fibrosis of the conjunctiva.
It may also be useful in glaucoma because one of the primary problems glaucoma surgeons face when patients need to have a conjunctival filtering bleb is that those procedures can fail by fibrosis caused by myofibroblasts. When using tubes, those can fail by myofibroblasts causing encapsulation of the tube. Losartan could penetrate the conjunctiva and be effective for those, he said.
He noted that it could be worth studying this as an option for proliferative vitreoretinopathy, which can occur in patients who have retinal detachments or diabetes, because that involves myofibroblast-driven fibrosis affecting the retina and vitreous. Extended delivery devices could potentially be studied as an option for giving losartan in these cases.
Further research is needed on the applications that Dr. Wilson is studying, as well as applications in other areas of ophthalmology. Instead of focusing on individual groups, Dr. Wilson wanted to encourage trials to ensure there is data to support the use and proper dosage. “We need the trials, but there are patients out there right now who can benefit from this treatment, and there are no reported complications,” he said.
When Dr. Wilson ends his lectures nowadays, he likes to reference his quest for the last 30 years to find a “magic bullet” to treat corneal fibrosis. “It was in my medicine cabinet all along,” he said, noting that he’s been on losartan for hypertension for around 20 years. He said it’s interesting that this drug that is so widely used for other things can be repurposed as such an incredible option for the cornea.
About the physician
Steven E. Wilson, MD
Professor of Ophthalmology
Director of Corneal Research
Cole Eye Institute
Cleveland Clinic
Cleveland, Ohio
References
- Wilson SE. Topical losartan: practical guidance for clinical trials in the prevention and treatment of corneal scarring fibrosis and other eye diseases and disorders. J Ocul Pharmacol Ther. 2023;39:191–206.
- Sampaio LP, et al. Topical losartan inhibits corneal scarring fibrosis and collagen type IV deposition after Descemet’s membrane-endothelial excision in rabbits. Exp Eye Res. 2022;216:108940.
- Sampaio LP, et al. Topical losartan and corticosteroid additively inhibit corneal stromal myofibroblast generation and scarring fibrosis after alkali burn injury. Transl Vis Sci Technol. 2022;11:9.
- Pereira-Souza A, et al. Topical losartan for treating corneal fibrosis (haze): first clinical experience. J Refract Surg. 2022;38:741–746.
Relevant disclosures
Wilson: Dr. Wilson and the Cleveland Clinic have submitted a patent on the use of topical losartan and other angiotensin II receptor blockers to prevent and treat corneal scarring fibrosis.
Contact
Wilson: WILSONS4@ccf.org