Cornea
April 2023
by Liz Hillman
Editorial Co-Director
When to refer, when to culture, treatment strategies, new treatment options, and more—EyeWorld spoke with Kenneth Beckman, MD, and Parag Majmudar, MD, to get an update on the latest in corneal ulcer management.
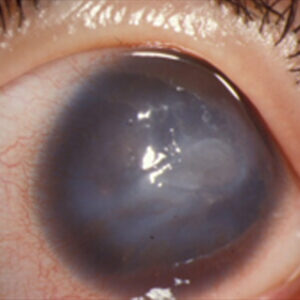
Corneal ulcers, Dr. Beckman said, typically present as an epithelial defect that develops a deeper infection into the stroma.
“They’ll usually present with staining in the area where the epithelium is gone and a white spot in the stroma,” Dr. Beckman said, noting that most patients with these will have a history of an abrasion, foreign body, contact lens wear, or even significant lid margin disease.
Causes
Dr. Majmudar categorizes corneal infections into four buckets: bacterial, fungal, viral, and other (atypical organisms, parasitic infections).
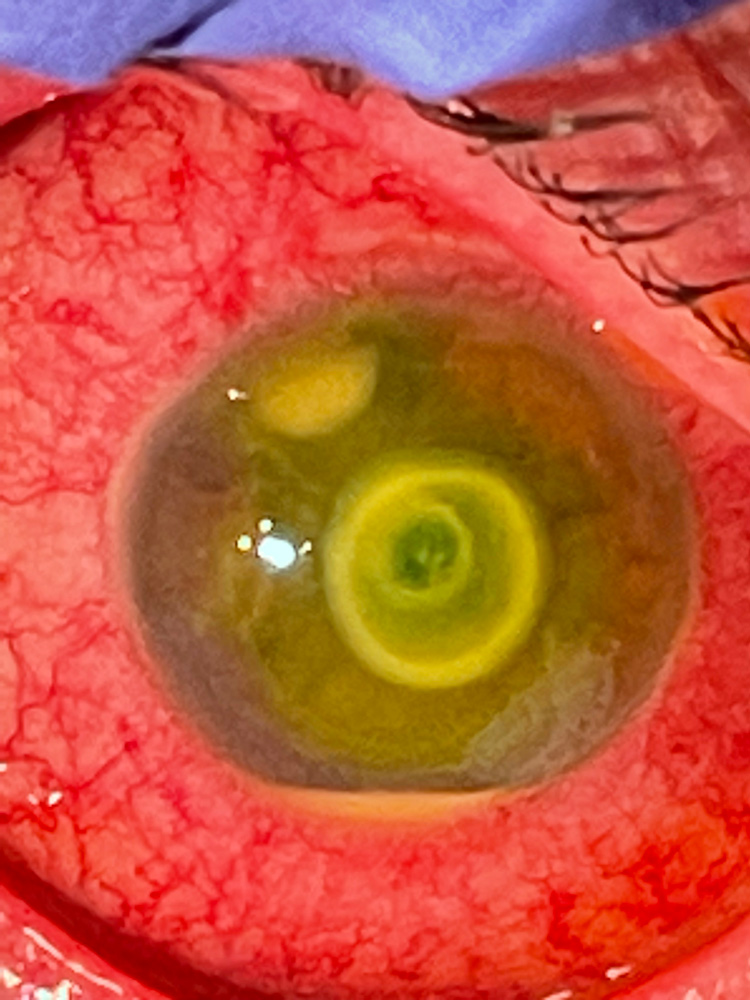
Source: Kenneth Beckman, MD
“Many times, the history and clinical presentation will give you some clue as to which category the infection falls into. For example, patients who use and/or abuse contact lenses are most likely going to experience bacterial infections,” he said. “Patients who are immunocompromised or live in tropical climates may have a higher risk of fungal infections. Viral infections are fairly ubiquitous, the most common being the herpes virus family, including herpes simplex as well as zoster, although technically zoster is more of an immunologic reaction than an active infectious one.
“Atypical organisms like mycobacteria are very rare. There was some increased incidence in post-refractive surgery patients in the late 1990s and early 2000s, but we don’t hear about that as much anymore,” Dr. Majmudar said. “Although parasitic infections are largely relegated to patients who have had exposure outside the U.S., one of the parasitic infections that continues to plague corneal specialists is Acanthamoeba. More often than not, there is a history of exposure to contact lenses and freshwater such as swimming in lakes, although tap water in many communities across the United States has also been shown to harbor Acanthamoeba.”
Dr. Beckman said that patients with lid margin disease are more likely to get bacterial infections, like Staph and Strep, but he noted that atypical things are more common in patients who wear contact lenses or those who have had previous ocular surgery or exposures. Fungal infections, for example, are more common if the patient has been exposed to vegetative matter, like tree branches.
Anecdotally, Dr. Beckman said there seems to be an increase in fungal infections.
“I’m not sure why. It could be they’re just growing more. It could be that people are using steroids more readily. I don’t know, but it seems like it’s a lot more common than it was when I first started practicing years ago.”
Care and culturing
Both Dr. Beckman and Dr. Majmudar said their corneal ulcer patients are generally referred from other eyecare providers.
“My advice would be that any central ulcer should be cultured in order to provide the most effective and appropriate antibiotic treatment to the patient. If the clinical course is not going well, I would recommend reculturing and expanding the culture to include other atypical organisms.”
Parag Majmudar, MD
“As a corneal specialist who practices in a tertiary care environment, the majority of ulcer patients who I see have already seen one or more eyecare providers. More often than not, they have had multiple prior treatments and may not be improving,” Dr. Majmudar said.
He said his rule of thumb for referrals is “if you don’t think that you can provide the most appropriate and efficacious care for that patient, send them to someone who can do so.” However, he thinks most corneal ulcers can be effectively managed by non-cornea specialists with a basic understanding of common pathogens in the region and appropriate antibiotic therapy.
“A pet peeve of mine is if a patient presents with a presumed contact lens-related infection, treatment should generally be directed toward Pseudomonas,” Dr. Majmudar said. “I’ve seen many patients be treated and ultimately referred to me for failed treatment, but they have been on antibiotics that have very little gram-negative coverage.”
Both physicians said that they culture almost all patients with a few exceptions. Dr. Majmudar said he might not culture if the lesion is not too peripheral or small.
“My advice would be that any central ulcer should be cultured in order to provide the most effective and appropriate antibiotic treatment to the patient. If the clinical course is not going well, I would recommend reculturing and expanding the culture to include other atypical organisms.”
Dr. Beckman said he’ll try to get a culture before antibiotic therapy begins because it can limit the yield of the culture. If that’s not possible, he’ll still get a culture because there will sometimes still be a yield. He also mentioned that if the patient wears contacts and has them in the case, they can be used to culture, or he said that a corneal biopsy could get a specimen if initial cultures remain negative.
“In some infections where cultures remain negative and they are not responding to treatment, if the infection is very deep, I may take a suture and pass it through the stroma, through the cornea mid-depth, not into the anterior chamber … so that it tracks deep enough so that I might get a better specimen and use that to culture,” he said.
While Gram stains can come back within a day, bacterial cultures can take 3–4 days, and fungal cultures can take a month. Dr. Majmudar pointed out that there are several labs that do PCR testing on a number of pathogens with a swab, rather than culture plates, which he said makes it relatively easy for any practice to do.
Treating
Dr. Beckman will usually start patients on aggressive antibiotics, a fourth-generation quinolone or fortified antibiotic drops, even if the culture hasn’t come back with a specific pathogen yet. Some patients, depending on severity, will be instructed to use this every hour. Also depending on severity, patients are followed up within the clinic every day or two. Once the epithelium heals, Dr. Beckman said he’ll cut back on treatment but will keep them on drops for a couple of weeks. Antibiotics may be tailored more specifically once the culture comes back. If the culture comes back as a fungus, he’ll begin an antifungal but will also keep them on the antibiotic. If quinolone monotherapy was used initially and isn’t effective, Dr. Beckman said he’ll move on to a combination of fortified antibiotics.
Dr. Majmudar said the most commonly prescribed antibiotic for corneal ulcers is moxifloxacin, but it has limited gram-negative coverage. He will start a patient on broad-spectrum fortified antibiotics, including fortified cefazolin or vancomycin and fortified tobramycin. Fungal treatment is dependent on whether it is filamentous or yeast. He said as a primary intervention he would use voriconazole or natamycin for filamentous fungal infections and amphotericin B for yeast infections.
Dr. Beckman said he does not typically use steroids, though he thinks a lot of other physicians do. Steroid use for corneal ulcers has been debated. The Steroids for Corneal Ulcers Trial found that “adjunctive topical corticosteroid therapy may be associated with improved long-term clinical outcomes in bacterial corneal ulcers not caused by Nocardia species.”1
“If one is going to use a steroid, you want to see there is clear improvement with antibiotics before you do it. Those signs would be the epithelium healing, the infiltrate consolidating, any inflammation going away, the anterior chamber (if there are cells) resolving, improved redness, improved comfort, and it really helps if you identified the bug on the original cultures,” Dr. Beckman said.
Dr. Majmudar also said he likes to see some sort of clinical progress before starting steroids, but he’ll use them after 3–4 days in a compliant patient.
ARTICLE SIDEBAR
Three tips for corneal ulcers from Dr. Beckman
- Get a history. Always ask about injury, foreign body, contact lens wear, and exposure. “If there is something unusual, then you have to think of unusual things.”
- Watch patients closely. Look for signs of improvement. Use caution with steroids. If there is secondary inflammation that you have to treat, it’s best to do so once you have the infection under control and know it’s not fungal.
- Get the epithelium to heal quickly. If a patient isn’t healing, it doesn’t necessarily mean they need more antibiotics. Sometimes it means you need less. Some fortified antibiotics are harsh and can result in a persistent epithelial toxicity.
ARTICLE SIDEBAR
What about crosslinking?
Over the last few years there have been studies and reports of crosslinking as a possible therapy for corneal ulcers caused by fungal infections. While these results have been “generally positive,” Dr. Majmudar said, they’re mixed.
And it’s expensive. In the U.S., for example, Dr. Beckman said crosslinking for this indication would not be covered by insurance, and the riboflavin alone costs several thousand dollars.
“It also doesn’t seem necessary. For a fungal infection, we have a lot of antifungals out there and they may do well. I’m not convinced from the data that it would be better. It seems like a last resort to potentially avoid a transplant.”
On that note, Dr. Majmudar said that he thinks it may play a role in recalcitrant ulcers that would otherwise require a corneal transplant.
About the physicians
Kenneth Beckman, MD
Comprehensive Eyecare of Central Ohio
Westerville, Ohio
Parag Majmudar, MD
Associate Professor of Ophthalmology
Rush University Medical Center
Chicago, Illinois
Reference
- Srinivasan M, et al. The Steroids for Corneal Ulcers Trial (SCUT): secondary 12-month clinical outcomes of a randomized controlled trial. Am J Ophthalmol. 2014;157:327–333.
Relevant disclosures
Beckman: None
Majmudar: None
Contact
Beckman: kenbeckman22@aol.com
Majmudar: pamajmudar@yahoo.com