Glaucoma: Complicated cases
December 2021
by Ellen Stodola
Editorial Co-Director
A tube shunt erosion or exposure is a complication that can occur oftentimes many years after surgery. Several experts discussed what to look for, why this complication occurs, and how to address it.
Jonathan Myers, MD, noted there is about a 5–8% risk of a tube shunt erosion requiring a repair in the long run.1 It’s not rare, he said, but it’s infrequent enough to be overlooked, especially since it’s often many years after surgery.
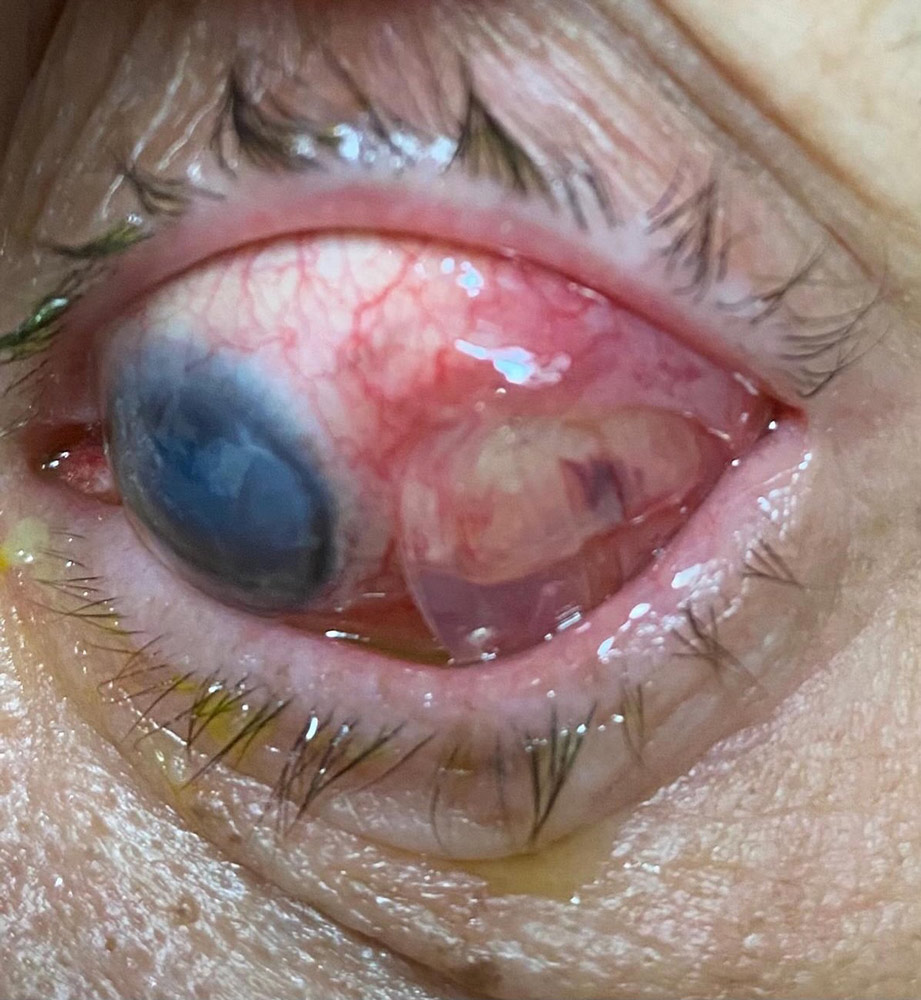
Source: Reza Razeghinejad, MD
The most concerning cases are the ones where infection ensued, and what’s been most interesting is the vast majority of erosions don’t involve infection, he said. “It’s relatively uncommon to have a tube shunt-related infection,” Dr. Myers said. “But usually when you do, there’s an erosion.”
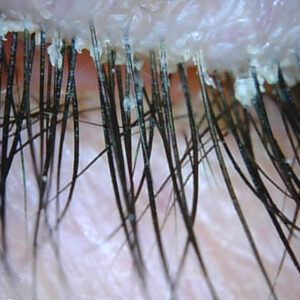
Most patients are asymptomatic or may have a little irritation under the eyelid. Sometimes an erosion is small (half a millimeter), while other times it has clearly been eroding for months and is larger (3–5 mm or even more), Dr. Myers said.
Dr. Myers noted that there are a couple of risk factors for tube shunt erosion. Patients with a Boston KPro (Massachusetts Eye and Ear) seem more at risk. “They have surface issues, are on chronic steroids, and often wear contact lenses,” he said. “I do think it’s more common to have an erosion in that setting.”
He noted a study by researchers at Duke University,2 who published a series on tube shunts, indicating that patients with multiple anti-VEGF injections for macular degeneration and related issues were more likely to experience tube shunt erosions.
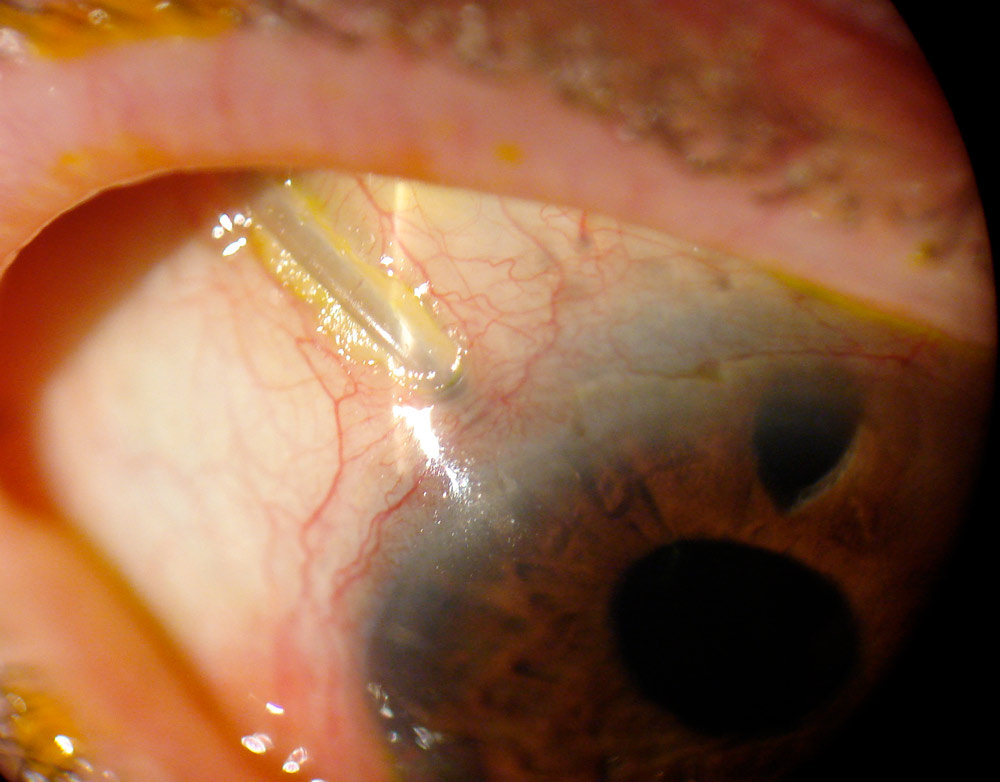
According to Oluwatosin Smith, MD, tube exposure is one of the more common complications that can occur following tube shunt surgery. In the Tube Versus Trabeculectomy study, tube erosion occurred in 5% of patients in the tube shunt group with some of the patients having a recurrence.3 “It can occur early on, which may be related to surgical technique, or further along after the patient has had the tube for many years,” she said. The tube exposure can occur along the tube itself or along the plate of the drainage implant.
Dr. Smith said some factors associated with tube erosion include location of the tube, positioning, the point of entry into the eye, and a patient’s history of other ocular surgeries or systemic disease. She also mentioned cases where the tube was exposed after trauma following a retina injection close to the tube. The possibility of exposure should be kept in mind when implanting a tube. It’s important to make sure the tube itself is covered by the eyelid at the pressure points and points where it enters the anterior chamber, she said. This is key, hence her tendency to enter the anterior chamber at 12 o’clock and at least 2 mm posterior to the limbus.
Reza Razeghinejad, MD, said that tube exposure can be divided into two groups: early tube exposure and late-onset tube exposure.
Early tube exposure, he said, is often caused by a dehiscence of the suture that secures the conjunctiva or conjunctival retraction and dehiscence due to having tension on the conjunctiva.
The exact mechanism for late-onset tube exposures is not known, Dr. Razeghinejad said. It’s likely related to an erosion of the overlying conjunctiva and patch graft due to the micro- movements of the tube with blinking and eye movements, he said.
The reported risk factors for tube exposure are ocular inflammation, neovascular glaucoma, increased number of preoperative glaucoma medications, diabetes mellitus, prior ocular surgeries with conjunctival violation (strabismus surgeries, retinal detachment surgeries, pterygium surgery with free conjunctival flap, etc.), and inferiorly implanted tubes.4–7
Late tube exposure is estimated to occur in 2.5–8.9% of patients and commonly more than 1 year postoperatively.4–7 “As I work in a tertiary eyecare center, I get these patients every month,” Dr. Razeghinejad said. “If you are in a private practice, you won’t see as many as I see and manage.” When tube exposure occurs, prompt surgical revision is highly recommended to prevent endophthalmitis, he added.
Dr. Razeghinejad noted that he operated on a patient with a re-exposure who had intravitreal injection and tube revision by her surgeon for tube exposure and endophthalmitis 4 weeks prior. “She had cells in the anterior chamber and exudates around the intracameral portion of the tube,” he said. The retina colleagues recommended tube explantation because they thought the tube was infected. The cause of the tube exposure, he said, was anterior tube insertion, which was not addressed in the first tube revision. In the second revision surgery, Dr. Razeghinejad cut the anterior portion of the tube and used a tube extender and inserted it more posteriorly around 12 o’clock. A cornea patch graft was used.
Planning and prevention
Source (all): Oluwatosin Smith, MD
Dr. Smith noted that tube exposure is generally easy to spot when patients come in for routine visits, and she stressed the importance of actively checking when patients come in. “Being constantly aware that this is possible is one of the important things as you follow patients who have had tube shunts,” she said.
Dr. Smith also said she is careful to advise patients who get repeated retinal injections to remind the retinal surgeon about the placement of the tube. Just being alert to the location of the tube is important, she said.
To try to plan for this and prevent it from occurring, Dr. Razeghinejad suggested inserting the tube at least 2 mm posterior to the limbus. He also said to have no tension on the conjunctiva when you close it; you may need to undermine the conjunctiva and have the loose conjunctiva covering the whole area of bare sclera before suturing. If you are pulling the conjunctiva toward the limbus with the aid of suture force, Dr. Razeghinejad said there is a good chance that you may get patch and tube exposure.
Dr. Myers said that he has used patch grafts in primary surgery to prevent erosions. However, these often dissolve over time.
“For those of us who switched to long intrascleral tunnels for tube insertions, it seems the erosions are less common with intrascleral tunnels without patch grafts,” he added, noting that there is not a lot of data to know for sure. “But I haven’t seen a case yet of an erosion in a patient with a long scleral tunnel, 5 mm or more, without a patch graft.” The switch to this approach has been more recent. “A lot of us switched to that when CMS stopped reimbursing the surgery center for patch grafts,” he said. “I think that was about 3 years ago, and since it often takes years to develop an erosion, I’m not sure if I can say that definitively makes a difference.”
Managing the complication
If it’s in the early postop period, Dr. Razeghinejad said revision surgery is mandatory if the tube is exposed. If the patch is exposed and still covering the tube, topical antibiotics and lubricants (drops and gels) usually help with conjunctivalization of the patch, he said.
With late tube exposure, Dr. Razeghinejad said the need for revision is urgent because the chance of endophthalmitis is high.
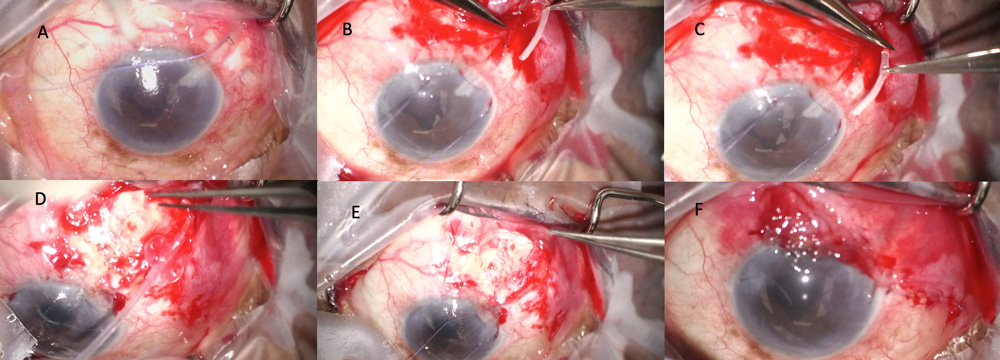
The conjunctiva around the area of the tube exposure is usually friable and congested. “I do inject lidocaine plus epinephrine to balloon the conjunctiva and decrease the bleeding,” he said. “It also helps me to delineate the boundaries of free and scarred conjunctiva. I dissect the conjunctiva posteriorly, and due to the tissue expansion effect of the plate on the conjunctival tissue, there is enough conjunctiva over the plate to undermine and pull forward toward the limbus.”
Generally, Dr. Razeghinejad said the conjunctiva at the area of tube exposures is not a good tissue to cover the new patch and tube, and it’s necessary to bring fresh conjunctiva from superior or the sides to close the defect area. He added that free conjunctival grafts or rotational flaps, double-layer amniotic membranes, and buccal membrane transplants may be used for superficial coverage in the event of conjunctival scarring.4,8
If the tube is inserted anteriorly (close to the limbus or at the limbus), Dr. Razeghinejad prefers to relocate it more posterior and close the original tube entry with Vicryl sutures. “When you close the tract, you have to over tighten the suture to stop the leak, which usually leads to astigmatism,” he said. “Vicryl sutures dissolve within 4–6 weeks, but nylon lasts longer and you have to deal with the astigmatism postoperatively if you use nylon sutures.”
When you see the tube is exposed, whether it’s the plate or tube itself, Dr. Smith said it’s important to start antibiotics, manage the early infection if present, and seek the help of a retina specialist if indicated as in the case of endophthalmitis.
The approach to an exposed tube also depends on what section of the tube is exposed, she said.
If the plate is exposed, the whole tube usually has to come out because it’s hard to get the plate covered after the capsule is violated due to epithelialization within it.
However, if it’s tube exposure over the tubing material, Dr. Smith said the approach is usually to go in and open the conjunctiva. “It’s important to cauterize any epithelial tissue that would have grown into and around the tube subconjunctivally.” Conjunctival closure may be a challenge in certain instances, so tissue mobilization, the use of amniotic membranes, conjunctival graft, or pedicle flap are ways of achieving adequate coverage.9
“When we think about exposed hardware in other parts of the body, often they remove that hardware. In most cases, even those cases of infection, we don’t remove or replace the tube.”
Jonathan Myers, MD
Dr. Smith said she tends to move the tube position as well because she thinks there is some mechanical effect that has a part to play in why the tube was exposed in that location. She usually moves the tube over about one clock hour toward 12 o’clock. Snaking and securing tube material during primary tube surgery as she directs the tube to the 12 o’clock position leaves extra tubing available for relocation of the entry point in the future if this is needed.
Patch graft material or method is another discussion, she said. Whether you put a patch graft or create a long track for the tube as it enters the eye, as you revise, you should try to use patch material to cover the tube to prevent re-exposure.
Most patients do well with tube revision. There are some extreme instances with severe infection or where the tube is completely expelled in which vision is significantly threatened, Dr. Smith said, but in most instances, patients recover fully following a revision with maintenance of pre-exposure IOP if it was just an exposed tubing.
“When we think about exposed hardware in other parts of the body, often they remove that hardware,” Dr. Myers said. “In most cases, even those cases of infection, we don’t remove or replace the tube.” If tube position is good in the anterior chamber and on the sclera, and if it’s not too close to the limbus, the surgeon can patch over the tissue and reclose the conjunctiva and not have another erosion in the vast majority of cases.
“If we see something that predisposes to erosions, like the tube shunt is a little too anterior in insertion or if it has a laxity to it so the tube bows up, most of us would reposition,” Dr. Myers said. “But for most of the patients, another patch graft on top, deepithelialize the area with cautery, and make sure that fresh conjunctiva is brought down that’s not under tension.” Even with long-term follow up, it’s rare the patient gets a second erosion, he said, though he noted it can happen.
“I think in any patient who has an infection and erosion, you have to assume it’s from the erosion,” Dr. Myers said. The erosion is usually easy to identify, but he added that non-glaucoma specialists may not be specifically looking for this.
Dr. Myers added that the further back from the limbus that the tube is inserted, the less likely it is to have erosion. A tube that’s placed in the sulcus, in general, tends to enter the eye more posterior. A tube in the pars plana is even more posterior. “When it doesn’t extend as far anterior to the limbus, I think the risk of erosion is much smaller,” he added.
Dr. Myers said it’s always a balance of pros and cons. People with good tissue do better, and the better the placement, the better they tend to do, but there are some patients who still run into problems. Eyes that had prior surgery and those with tissue and surface issues are more at risk as well, he said. Careful vigilance in eyes with prior tube shunt surgery will identify erosions early before serious problems arise in most cases.
About the physicians
Jonathan Myers, MD
Chief of the Glaucoma Service
Wills Eye Hospital
Philadelphia, Pennsylvania
Reza Razeghinejad, MD
Director
Glaucoma Fellowship Program
Wills Eye Hospital
Philadelphia, Pennsylvania
Oluwatosin Smith, MD
Glaucoma Associates of Texas
Dallas, Texas
References
- Trubnik V, et al. Evaluation of risk factors for glaucoma drainage device-related erosions: A retrospective case-control study. J Glaucoma. 2015;24:498–502.
- Liu KC, et al. Recurrent tube erosions with anti-vascular endothelial growth factor therapy in patients with age-related macular degeneration. Ophthalmol Glaucoma. 2020;3:295–300.
- Gedde SJ, et al. Postoperative complications in the Tube Versus Trabeculectomy (TVT) study during five years of follow-up. Am J Ophthalmol. 2012;153:804–814.
- Oana S, Vila J. Tube exposure repair. J Curr Glaucoma Pract. 2012;6:139–142.
- Chaku M, et al. Risk factors for tube exposure as a late complication of glaucoma drainage implant surgery. Clin Ophthalmol. 2016;10:547–553.
- Muir KW, et al. Risk factors for exposure of glaucoma drainage devices: a retrospective observational study. BMJ Open. 2014;4:e004560.
- Levinson JD, et al. Glaucoma drainage devices: risk of exposure and infection. Am J Ophthalmol. 2015;160:516–521.
- Einan-Lifshitz A, et al. Repair of exposed Ahmed glaucoma valve tubes: long-term outcomes. J Glaucoma. 2018;27:532–536.
- Grover DS, et al. Forniceal conjunctival pedicle flap for the treatment of complex glaucoma drainage device tube erosion. JAMA Ophthalmol. 2013;131:662–666.
Relevant disclosures
Myers: Aerie, Avisi, Allergan, Equinox, Glaukos, Guardion Health Sciences, Haag-Streit, MicroOptx, Nicox, Olleyes, Santen
Razeghinejad: Olleyes
Smith: New World Medical
Contact
Myers: JMyers@willseye.org
Razeghinejad: razeghinejad@yahoo.com
Smith: tsmith@glaucomaassociates.com