Refractive: Complicated cases
December 2021
by Ellen Stodola
Editorial Co-Director
Sometimes after initially picking a treatment option, a patient’s vision can change over time, requiring another solution. Luke Rebenitsch, MD, described a case where he initially performed same-day hyperopic LASIK along with the KAMRA inlay (SightLife Surgical) for distance and presbyopia correction, respectively, in a 46-year-old patient. Several years later, Dr. Rebenitsch elected to implant IOLs in the patient once he started experiencing a hyperopic shift and lens-associated degradation in vision. The patient was satisfied with both his distance and near vision.
Dr. Rebenitsch noted that when he first saw this patient in 2017, he was a 46-year-old carpenter who was hyperopic and desired both distance and near vision. The patient’s main goal was to gain independence from glasses.
After discussion with the patient, the plan was made to perform bilateral hyperopic LASIK, targeting plano in the right (dominant) eye, and a –0.75 D in the left (non-dominant) eye. The left eye also received the KAMRA inlay.
At the 1-month postoperative visit, the patient’s UDVA was 20/12 in the right eye and 20/30 in the left eye, with UNVA at 20/30 as well. Fully healed 5 months later, his UDVA was 20/10 in the right eye, 20/25 in the left eye, 20/10 both eyes, and UNVA was 20/20.
The patient enjoyed this level of vision until earlier this year, when he returned with complaints of reduced near vision. His UDVA was 20/20 in the right eye and 20/25 in the left. However, his UNVA was reduced to 20/50, and this was significantly limiting his quality of life.

“Upon refraction, we found he had drifted hyperopic, which is common for a 50-year-old, to +0.75 in the right eye and +1.25 in the left eye, which would explain the loss of near vision,” Dr. Rebenitsch said.
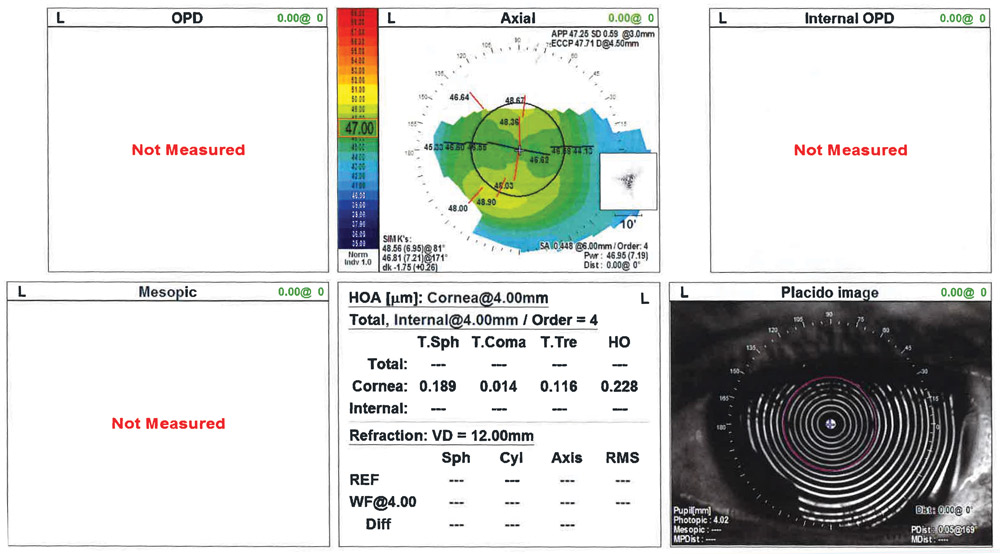
This patient’s goal was to obtain the most permanent vision correction procedure possible. Given the patient’s current complaints, age, and diagnostic testing, the decision was made to do a refractive lens exchange in both eyes. The topography and higher order aberrations were within normal limits, Dr. Rebenitsch said, so he discussed with the patient the option of doing a multifocal lens in the dominant eye and a monofocal lens behind the existing KAMRA.
“He understood that there was an increased risk of halo and glare, but he wanted to have distance and near in both eyes,” Dr. Rebenitsch said.
Dr. Rebenitsch used a TECNIS ZKB00 (Johnson & Johnson Vision) +2.75 add in the right eye and a ZCB00 single focus lens in the left eye. At his 1-day postoperative exam, the patient was ecstatic. At 1 month after surgery, Dr. Rebenitsch said the patient still noticed some minor light sensitivity and foggy vision but now has vision better than he had with the KAMRA inlay initially.
Dr. Rebenitsch shared several takeaways from this case. First, it’s expected that patients will drift hyperopic. Even though the KAMRA inlay target is between –0.75 and –1.0 D, you will lose some of that depth of focus as people naturally drift more hyperopic and become more presbyopic.

Source (all): Shehzad Batliwala, DO, and Luke Rebenitsch, MD
Dr. Rebenitsch said this case highlights the fact that in some instances, multifocal lenses can be a great option in post-hyperopic LASIK patients. The surgeon must ensure that the cornea is pristine with acceptable spherical aberration and minimal higher order aberrations. A well-centered ablation is critical.
Dr. Rebenitsch noted that many surgeons have stopped using inlays. Because of the natural hyperopic drift over time, some patients are coming back several years after their inlay procedures and are looking for a more permanent solution, he explained. Additionally, Dr. Rebenitsch said that he thinks multifocal lenses have achieved such a great level of quality that he typically opts for a RLE rather than an inlay.
Shehzad Batliwala, DO, shared some thoughts on the case. He said he thinks it’s important to note how this case demonstrates the advancement of modern LASIK in terms of the lasers and ablation profiles used to minimize optical aberrations. “We were still able to put a multifocal lens in this patient after having had hyperopic LASIK, which, 10–15 years ago, was unheard of,” Dr. Batliwala said. “As excimer lasers have improved their optics, this has allowed us to continue to use multifocal lenses in these types of patients.”
About the physicians
Shehzad Batliwala, DO
Surgery Fellow
ClearSight LASIK/43 Vision
Oklahoma City, Oklahoma
Luke Rebenitsch, MD
Medical Director
ClearSight LASIK/43 Vision
Oklahoma City, Oklahoma
Relevant disclosures
Batliwala: None
Rebenitsch: Carl Zeiss Meditec, Legrande, OSRX Pharmaceuticals, STAAR Surgical
Contact
Batliwala: shehzad@drbatliwala.com
Rebenitsch: Dr.Luke@ClearSight.com