ASCRS News
December 2021
The Ophthalmology Quicksand Chronicles podcast, hosted by Elizabeth Yeu, MD, and Nicole Fram, MD, features experts sharing their “quicksand moments” in the OR, lessons learned from those moments, and how these vulnerable situations ultimately helped them evolve as surgeons.
“The Unrelenting Uveitic Cataract”
Zaina Al-Mohtaseb, MD, joined Drs. Fram and Yeu to share her “quicksand moment” with a uveitic cataract, a teaching case with Dr. Al-Mohtaseb’s resident who began the case.
This particular patient had no medical history or background information, so this made it challenging to know how long the problem had persisted.
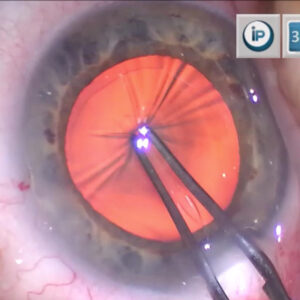
The patient had significant posterior synechiae, and the resident started by trying to make an opening to lift up the iris that was stuck on the anterior capsule with a white cataract. The pupil in this case was very small.
Early on, Dr. Al-Mohtaseb made marks on the eye for iris hook placement. “Surgery is about thinking ahead and trying to avoid complications,” she said. An important aspect is to ensure you have all the instruments and supplies you’ll need in the operating room. Dr. Al-Mohtaseb mentioned having epinephrine for dilation, trypan blue, a 23- or 25-gauge Maxgrip forceps, intraocular scissors, tools for anterior vitrectomy, a Yamane kit, and CTR segments.
The case was proceeding as planned, with a dark brown appearance that she thought was pigment left behind. The resident was using I/A to remove OVD in order to stain the capsule and get a better view, and Dr. Al-Mohtaseb began to realize that rather than remnant pigment, the iris had split, and it was remnant membrane.
At this point, Dr. Al-Mohtaseb took over the case. The membrane was fibrotic and there was a big space between the membrane and anterior capsule below. She knew that she would need to use anterior vitrectomy to get rid of the membrane.
Dr. Al-Mohtaseb agreed with a point made by Dr. Yeu that often the synechiae may actually be keeping the capsule in place when there are no zonules. It’s important to remove enough synechiae to see but to leave some.
There was no support and no tension from any remaining zonules. It was very leathery and even cutting was tough. She wanted to make a small opening in order to remove the cataract because it was very dense. She used anterior vitrectomy and decreased the cut rate to make an opening in the anterior capsule.
She wanted to get the nucleus out safely and decided not to utilize the bag. She noted that there is no long-term data on patients with uveitic cataracts and intrascleral fixation. She also said that the possibility of using Gore-Tex sutures made her nervous in this patient, so she decided against it. She had to think if it was better to leave this monocular patient aphakic and not try to preserve the bag, which is what she ultimately decided to do.
“This was a case where I didn’t have all the answers,” she said. There were certain things she was trying to accomplish, namely not losing nuclear material in the back of the eye and trying not to cause retinal tears.
The age of the patient is also a factor in the decision-making process. For a younger patient, Dr. Al-Mohtaseb said she might be more likely to try to save the bag but thought her chosen option was good for this older patient.
After addressing the remnant material, Dr. Al-Mohtaseb discovered that the patient also had a vitreous hemorrhage underneath. At this point, she was wondering about doing Yamane vs. leaving the patient aphakic. But when she saw the vitreous hemorrhage, she thought it would be better to leave the patient aphakic and see what the visual potential was and if there was inflammation. Dr. Al-Mohtaseb said this case demonstrates how a surgery can involve a decision tree of tough choices.