Cover Feature: Navigating the red eye
May 2018
by Michelle Stephenson
EyeWorld Contributing Writer
Hyperacute bacterial conjunctivitis requires prompt diagnosis and treatment because some types, specifically conjunctivitis caused by Neisseria gonorrhoeae or Neisseria meningitides, can cause corneal ulceration, corneal opacification, corneal perforation, and panophthalmitis. These organisms can also potentially cause a secondary meningitis, which can be life-threatening.
“Less severe than hyperacute bacterial conjunctivitis, acute bacterial conjunctivitis is primarily due to Staphylococcus aureus, Streptococcus pneumoniae, and Haemophilus influenzae,” said Vincent de Luise, MD, New Haven, Connecticut. “Other pathogens responsible for acute disease are Pseudomonas aeruginosa, Moraxella lacunata, Streptococcus viridans, and Proteus mirabilis. These organisms may be spread from hand to eye contact or through adjacent mucosal tissues colonization, such as nasal or sinus mucosa.”
The most common acute bacterial conjunctivitis pathogens are Streptococcus pneumoniae, Haemophilus influenzae, and Staphylococcus aureus. Infections with S. pneumoniae and H. influenzae are more common in children, whereas S. aureus most frequently affects adults.
Chronic conjunctivitis is primarily due to Chlamydia trachomatis. However, chronically ill or immunocompromised patients can become colonized with other virulent bacteria responsible for chronic conjunctivitis. Staphylococcus aureus and Moraxella lacunata may also cause chronic conjunctivitis in patients with associated blepharitis.
“Hyperacute bacterial conjunctivitis is primarily due to Neisseria gonorrhoeae, which is a sexually transmitted disease,” Dr. de Luise said. “Neisseria meningitidis can also cause hyperacute bacterial conjunctivitis and can lead to potentially fatal meningeal or systemic infection.”

Source: Vincent de Luise, MD
Diagnosis
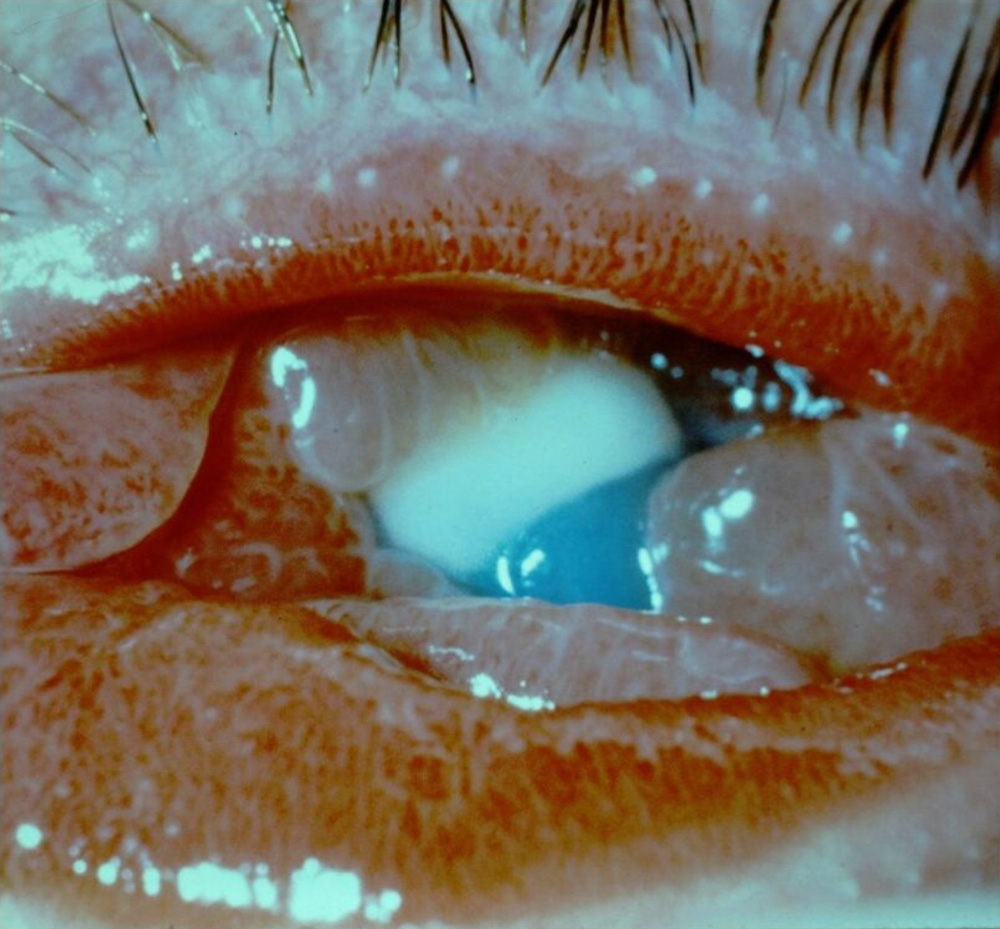
According to Francis Mah, MD, La Jolla, California, “Hyperacute bacterial conjunctivitis is accompanied by a copious amount of green or gray mucus. If you take a tissue and wipe some of it away, it is back immediately. It is typically unilateral, although it can be bilateral. There can also be significant eyelid edema and redness of the eye.”
According to Dr. de Luise, this condition is so dramatic that it can’t be mistaken for another condition. “It’s an explosive, rapid onset, severely purulent, pussy conjunctivitis. The patient comes to you and is weeping yellow discharge. I’ve seen it a few times in my career, but thankfully not very often. There are three things to remember when you see hyperacute bacterial conjunctivitis: It’s sight-threatening, it’s potentially life-threatening if it’s not treated immediately, and it requires systemic treatment and hospitalization. Gonococcus and meningococcus, which are the bacteria that cause this hyperacute conjunctivitis, can lead to corneal ulceration or corneal perforation, which can lead to endophthalmitis, or what we call a panophthalmitis, meaning every layer of the eye is inflamed,” he said.
The causes of hyperacute bacterial conjunctivitis are almost always bacteria in the genus Neisseria. “Neisseria gonorrhoeae or its cousin Neisseria meningitidis are often responsible,” Dr. de Luise said. “Neisseria gonorrhoeae is a sexually transmitted disease that would result from direct genital to eye contact or genital to hand to eye contact. It can also occur through maternal to neonate transmission during vaginal delivery. It is rare in neonates now because of the use of silver nitrate or erythromycin ointment on all neonates when they are born.”
Dr. Mah added that Neisseria gonococcus is one of the rare pathogens that can penetrate a normal, intact corneal epithelium. “Normally bacteria, viruses, fungi, and parasites can’t go through a normal cornea. They can only get in if there is a scratch, a defect, dry spots, or something abnormal on the cornea. Neisseria gonococcus can go through a normal, intact corneal epithelium, so it can cause an ulcer or a perforation. Other pathogens that can penetrate an intact cornea are Herpes simplex, Listeria, Neisseria meningitidis, and Acanthamoeba,” he said.
Dr. Mah noted that because Neisseria gonococcus is associated with a sexually transmitted disease, it is important to get the patient’s history in this regard. Patients should be asked whether they or their partner have a history of sexually transmitted diseases.
Source: Vincent de Luise, MD
Treatment
According to Dr. Mah, it is important to continue to remove the copious amounts of discharge because it contains Neisseria. “One of the main treatments is to irrigate and wipe the eye. Fluoroquinolone drops are also effective. Another component is systemic treatment. Azithromycin and doxycycline can be given orally. Patients with gonorrhea usually use ceftriaxone intramuscularly. If a patient is allergic to ceftriaxone, 2 g of azithromycin can be given orally in a single dose. Gentamicin drops could also be used, especially in younger children,” he said.
Dr. de Luise added that if the cornea is intact, the patient can be treated as an outpatient with intramuscular ceftriaxone, 1 g. If the patient has Neisseria gonorrhoeae, they would need to be treated with intramuscular ceftriaxone and oral azithromycin (1 g orally).
“If the physician diagnoses hyperacute bacterial conjunctivitis, this can be a sexually transmitted disease by Neisseria gonorrhoeae bacteria,” Dr. de Luise said. “One should be worried about Neisseria gonorrhoeae, which is the gonococcus, or rarely Neisseria meningitidis, which is the meningococcus that causes meningitis. Neisseria meningitidis can cause a panophthalmitis and subsequent meningitis, which can be life-threatening if not treated promptly.”
Patients with gonorrhea have a high risk of concomitant chlamydial disease. “It’s very common to have both,” Dr. de Luise said. “Ceftriaxone treats the gonococcus and the meningococcus, but does not treat chlamydia. Patients with chlamydia need to be given a second antibiotic, which is azithromycin, 1 g orally. That treats the chlamydia, and the ceftriaxone treats the Neisseria agent.” All sexual partners should be identified, contacted, and treated as well.
He noted that the cornea is involved in almost half of the cases of hyperacute bacterial conjunctivitis. “About 40% of the time, there is an ulceration or a perforation, which is a sight-threatening and life-threatening emergency. These patients need to be admitted to the hospital to an infectious disease service. These patients require intravenous ceftriaxone because the intramuscular route doesn’t work quick enough. They should be treated with intravenous ceftriaxone, 1 g IV every 12 hours for 3 days. Ceftriaxone is a cousin of penicillin, so if a patient has a penicillin allergy, we can use ofloxacin, 400 mg orally twice a day for 5–7 days, or spectinomycin 2 g intramuscularly for at least 3 days,” Dr. de Luise said.
He added that all patients with hyperacute bacterial conjunctivitis need to be treated for gonococcus and for concomitant chlamydial infection, just in case. “It takes a few days to prove this by culture, so we should give the patient 1 g orally. It’s a simple thing to do, very few people have reactions to it, and it kills the chlamydial piece of the puzzle. The chlamydia is not causing the hyperacute pus. That’s being caused by the Neisseria. Chlamydia is one of those things that happens to be there a lot in patients with gonorrhea, therefore you want to treat both,” Dr. de Luise said.
Concurrent chlamydial conjunctivitis is commonly seen and should be managed with one of the following:
- Azithromycin 1000 mg single dose
- Doxycycline 100 mg bid for 7 days
- Tetracycline 250 mg qid for 7 days
- Erythromycin 500 mg qid for 7 days
Ophthalmia neonatorum
This is conjunctivitis in neonates. The two major organisms responsible for ophthalmia neonatorum are Neisseria gonorrhoeae and Chlamydia trachomatis. Gonococcal ophthalmia neonatorum is caused by Neisseria gonorrhoeae. “Neonates also may have systemic manifestations, including rhinitis, stomatitis, arthritis, meningitis, anorectal infection, and septicemia,” Dr. de Luise said.
Treatment is topical erythromycin and intramuscular or intravenous ceftriaxone (25 mg/kg to 50 mg/kg, up to a maximum of 125 mg), according to Dr. de Luise. Prevention of conjunctivitis in neonates is through the use of 1% silver nitrate or 0.5% erythromycin ointment.
“There are limits to what you can give babies, but they can be given ceftriaxone, just like adults. While this is very uncommon in children, the doctor has to have his or her antenna up because you don’t want to miss it. This is a life-threatening disease in adults and children,” he said.
Editors’ note
Dr. Mah has financial interests with Novartis (Basel, Switzerland), Bausch + Lomb (Bridgewater, New Jersey), and Allergan (Dublin, Ireland). Dr. de Luise has no financial interests related to his comments.
Contact information
de Luise: vdeluisemd@gmail.com
Mah: Mah.Francis@scrippshealth.org


