ASCRS News: ASCRS/EyeWorld Journal Club
September 2021
by Hans Andrews, MD, Jordan Comstock, MD, Jennifer Lindsey, MD

Director for Resident Education
Department of Ophthalmology and Visual Sciences
Vanderbilt University
Medical Center
Nashville, Tennessee
In March 2020, COVID-19 placed an enormous stress on healthcare systems worldwide, and ophthalmologic cases were no exception. At the peak of the pandemic, many elective surgical services, including cataract surgery, were canceled. Ophthalmologists were confronted with empty offices and operating rooms. Fortunately, as new protocols were implemented, elective cases began to resume. Physicians and administrators have been plagued with the responsibility to reopen operative suites while also keeping patients and staff safe.
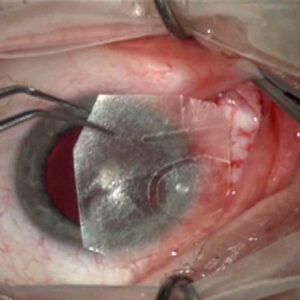
The idea that cataract surgery is an aerosol- generating procedure is up for debate. If aerosol is generated from the lens or aqueous material, this could result in the spread of COVID-19 in the operating room. The purpose of this study was to characterize and quantify the generation of aerosol in the operating theater during cataract surgery on human eyes.
The authors divided the study into two parts: a preliminary study and a follow-on study. In both parts, the authors included patients aged 50–80 who had visually significant cataracts and no other ophthalmic comorbidities. The preliminary study investigated 5 eyes of 3 patients, while the follow-on study had 20 eyes in 20 patients.

Ophthalmology Resident
Vanderbilt University
Medical Center
Nashville, Tennessee
The operating room used in this study had positive pressure ventilation and a high-efficiency particle filtration system. The study utilized a laminar airflow machine (LAF), which filters 99.995% of particles more than 0.3 mm and improves air sterility. A particle counter was used to detect any aerosolized particles by sampling the air over 21 seconds while reporting the cumulative number of particles in six different size categories ranging from <0.3 mm to <10 mm. During each operation, five intermittent measurements were taken before phacoemulsification and five during phacoemulsification.
The preliminary study set out to evaluate three main variables: (1) the effect of phacoemulsification on particle count, (2) the effect of LAF on particle count, and (3) the effect of OcuCoat (hydroxypropyl methylcellulose, Bausch + Lomb), a viscoelastic marketed to reduce aerosolization of particles, on particle count. These variables were tested on three patients. The first patient (one eye only) underwent standard cataract surgery with phacoemulsification comparing pre-phaco values to during phaco values. The second patient (eyes one and two) utilized the LAF machine for the entirety of the surgery on both eyes. The third patient (eyes one and two) utilized the LAF machine and OcuCoat viscoelastic.
The follow-on study evaluated 20 eyes with the use of the LAF machine and standard viscoelastic.
Results

Ophthalmology Resident
Vanderbilt University
Medical Center
Nashville, Tennessee
Baseline aerosol measurements were obtained in the operating room on two separate days, both before and after the LAF machine was turned on. There was no difference between day 1 and day 2, indicating no significant fluctuation in day-to-day measurements. Furthermore, there was no significant difference in particle size and quantity of particles with the LAF turned on or off.
In the preliminary study, there was no significant increase in particles before or during phacoemulsification in all five eyes of the three patients. When comparing patient 1 (no variables) to patient 2 (LAF on), there was a significant decrease in particles in both the pre-phaco and during phaco categories. This indicates a reduction in particle quantity when using the LAF machine. When comparing patient 2 (LAF on) to patient 3 (LAF on and OcuCoat), there was only a borderline difference between the second eye of each patient, which the authors concluded was more likely a cumulative effect of the LAF machine rather than the actual effect of OcuCoat. There was no difference in particle count between the first eye of patient 2 and patient 3, implying the use of OcuCoat does not significantly decrease aerosolization.
In the follow-on study of 20 eyes with use of the LAF machine and standard viscoelastic, there was significant reduction of particle size during phacoemulsification compared to pre-phacoemulsification. This implies that at least with the LAF machine turned on, there is no increase in particle count during phaco.
Discussion
Previous studies have suggested cataract surgery could be a potentially aerosol-generating procedure, yet the evidence is not definitive. A study on human cadavers demonstrated visible aerosol generation during phacoemulsification, however, a study on pig eye phacoemulsification did not show generation of aerosols.1,2 The findings of this study showed aerosol of less than 10 μm is not produced during phacoemulsification of the human lens under routine operating conditions. This supports the recommendations of the American Academy of Ophthalmology, which state the risk for aerosol generation during phacoemulsification should be very low.3 Furthermore, the results suggest that the use of OcuCoat does not significantly decrease the particle count and the LAF machine can be effective in decreasing overall particle count. The authors argued the risk of spreading live coronavirus from aerosolization in cataract surgery is low, and increased wait time between cases to decrease aerosol transmission is futile.
There were several limitations to this study. The sample size was small, especially in the preliminary study, limiting the overall power of the study. Furthermore, it is difficult to determine if these results can be universally applied at all surgical sites across the world, as the surgical techniques, like incision size or type of phacoemulsification machine, are not consistent across operating theaters.
During the ASCRS Journal Club discussion, members of the panel weighed in on how their personal practice patterns have changed in the COVID-19 era. The majority of the panelists had all elective cataract cases canceled following the initial rise of COVID-19 infections. Upon reopening, some of the panelists experienced longer turnover rates between surgical cases due to stricter decontamination protocols. Despite returning to pre-COVID surgical and clinical volume, all panelists maintained strict social distancing regulations in their waiting rooms and operative care units. The ASCRS Journal Club also discussed the mobile laminar air flow machine referred to in the article. None of the members of the panel have implemented this air flow system in their operating rooms. However, they all agreed a safe and effective air flow system in the operating room is imperative to prevent bacterial and viral infections, not limited to COVID-19.
As ophthalmologists resume the full spectrum of surgical cases, the COVID-19 pandemic continues to impact practice patterns, surgical decision-making, and overall safety measures. The panelists discussed how many patients remain hesitant to undergo elective surgery and attend clinic appointments. They agreed the results of this study provide reassurance to themselves, their staff members, and their patients that there is no significant aerosolization during phacoemulsification. We remain hopeful that the emergence of the COVID-19 vaccine will provide a further sense of security for patients.
Aerosol generation during phacoemulsification in live patient cataract surgery environment
Simerdip Kaur, MRCP, Nick Kopsachilis, MD, Rishid Zia, MRCSEd (Ophthal)
J Cataract Refract Surg. 2021;47(6):695–701
- Purpose: To investigate if phacoemulsification is an aerosol generating procedure in a live patient environment.
- Setting: New Hayesbank Ophthalmology Services, Kent, U.K.
- Design: In vivo experimental human eyes study
- Methods: We measured aerosol particle counts sized ≤0.3 µm, >0.3≤0.5 µm, >0.5≤1.0 µm, >1.0≤2.5 µm, >2.5≤5.0 µm, and >5.0≤10 µm during elective phacoemulsification surgery of 25 eyes. The baseline particle count in our operating theater was measured on 2 separate days to assess for fluctuation. Then we measured 5 readings each during pre-phacoemulsification and phacoemulsification of all eyes. We also measured the difference in aerosol generation during pre-phacoemulsification and phacoemulsification with the use of the mobile laminar air flow (LAF) machine. Lastly, we measured aerosol generation during phacoemulsification with the use of HPMC (2% hydroxypropyl methylcellulose).
- Results: There was no significant difference in measurement of aerosol between the baseline measurements on both days and between each patient’s pre-phacoemulsification and phacoemulsification stages of surgery. The LAF system showed statistically significant reduction in particles size of ≤0.3 µm, >0.3≤0.5 µm, >0.5≤1.0 µm, >1.0≤2.5 µm, >2.5≤5.0 µm, and >5.0≤10 µm during phacoemulsification compared to pre-phacoemulsification (t-test, p value 0.00 for all particle sizes). The use of HPMC (2% hydroxypropyl methylcellulose) did not show any statistically significant reduction in particle measurements.
- Conclusion: Aerosol particles sized <10 µm are not produced during phacoemulsification of human crystalline lens in a live patient setting. The use of a mobile laminar air flow (LAF) machine significantly reduced the number of particles sized ≤10 µm within the surgical field.
ARTICLE SIDEBAR
The ASCRS Journal Club is a virtual, complimentary CME offering exclusive to ASCRS members that brings the experience of a lively discussion of two current articles from the Journal of Cataract & Refractive Surgery to the viewer. Co-moderated by Nick Mamalis, MD, and Leela Raju, MD, the June session featured a presentation by David Belyea, MD, co-author of “The effect of eye drops and applanation tonometry on optical biometry.” The second manuscript, “Aerosol generation during phacoemulsification in live patient cataract surgery environment” was presented by Hans Andrews, MD, ophthalmology resident, Vanderbilt Eye Institute. To view the June Journal Club session, visit ascrs.org/clinical-education/journal-club/schedule/june-2021.
References
- Darcy K, et al. Reducing visible aerosol generation during phacoemulsification in the era of Covid-19. Eye. 2021;35:1405–1410.
- Lee H, et al. Aerosol generation through phacoemulsification. J Cataract Refract Surg. 2020;46:1290–1296.
- Chodosh J, et al. Special considerations for ophthalmic surgery during the COVID-19 Pandemic. 2020. American Academy of Ophthalmology.
Contact
Andrews: hans.w.andrews@vumc.org
Lindsey: jennifer.lindsey@vumc.org