Cataract
Summer 2024
by Ellen Stodola
Editorial Co-Director
The choice between using bimanual or coaxial I/A depends on a number of factors, including physician preference and the type of case. Rom Kandavel, MD, and Cristos Ifantides, MD, MBA, discussed what they use and what may be beneficial in certain cases.
Dr. Kandavel said that he has been in practice for 18 years, and initially, he began by using a mixture of bimanual and coaxial I/A. He came out of training primarily doing coaxial. In practice, his partner was primarily using bimanual. “After a period of acclimation, I switched over after I was convinced of the benefits of the technique.
“I will certainly use coaxial when I teach at different institutions, and there are hybrid models,” he said.
Dr. Ifantides uses both bimanual and coaxial I/A. “Very rarely will you find one instrument or technique that will work in every situation better than any other thing,” he said. “There’s no perfect technique or tool. We have to adapt to the scenario.”
Source: Cristos Ifantides, MD, MBA
Advantages of coaxial I/A
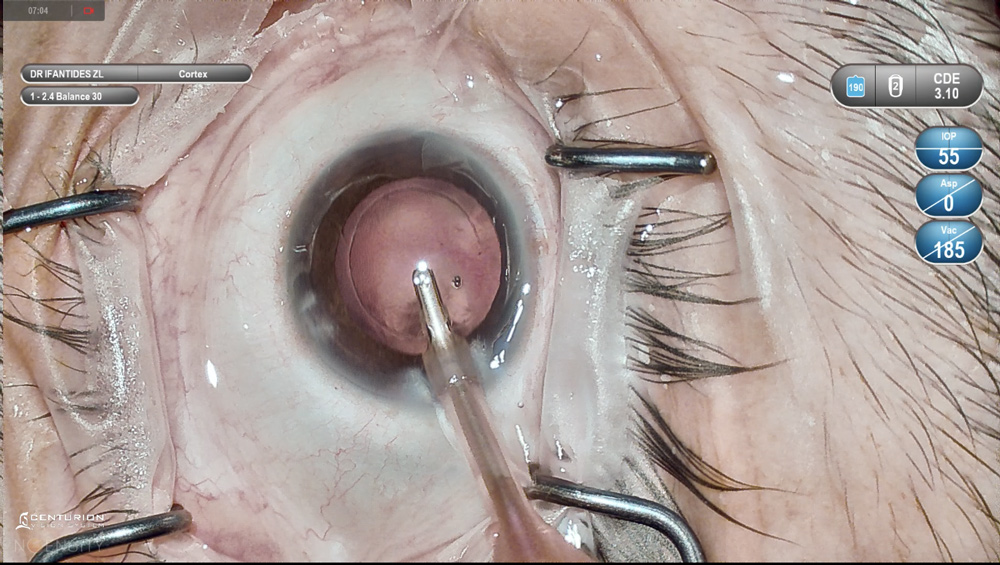
Dr. Ifantides said currently, his preference is to use coaxial I/A for several reasons. One is that other surgeons in his practice use this, so it’s about ease of use for the technicians. “The outcomes are very good, I can get access to everything I need, and I think it’s faster,” he said.
For routine cases and when pupil size and dilation are good, coaxial is best, Dr. Ifantides thinks.
Dr. Kandavel said he would choose to use coaxial I/A in some cases, specifically if he was averse to creating a second paracentesis. “There are not a lot of scenarios where you can’t fit a second paracentesis, but it could happen if the paracentesis was near a preexisting trabeculectomy or you have a large LRI,” he said.
It also depends on surgeon preference, and some surgeons don’t want to have another step. However, the time savings in not creating a second paracentesis could be made up by saving time during cortical cleanup, he said.
Source: Cristos Ifantides, MD, MBA
Advantages of bimanual I/A
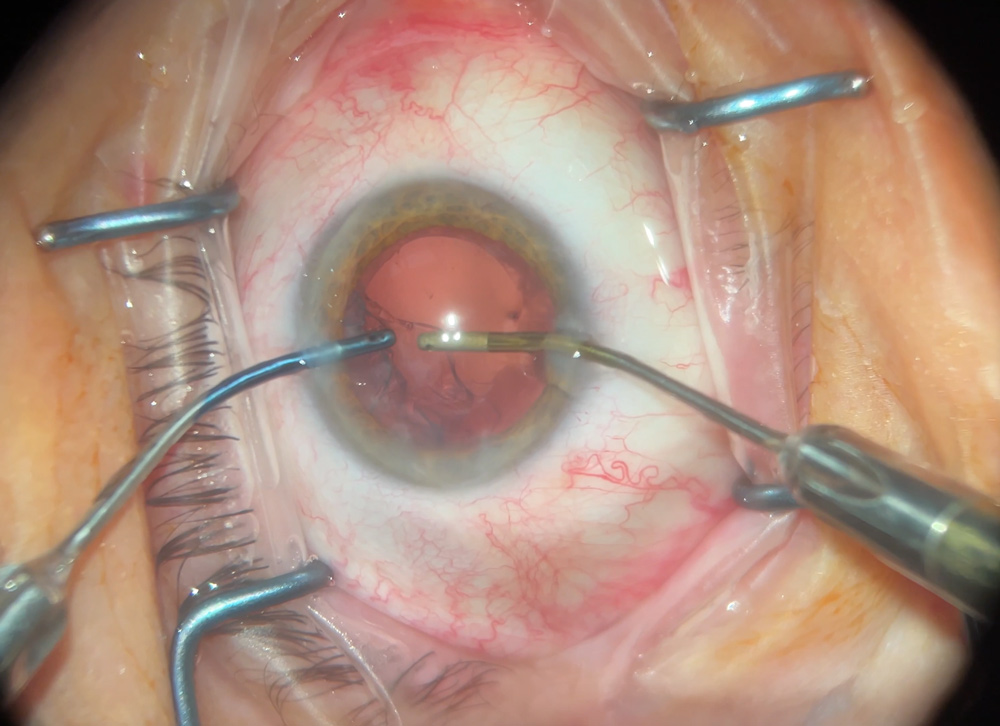
“I think the single biggest advantage is the dexterity and reach that bimanual I/A can afford for cortical cleanup and the chamber stability,” Dr. Kandavel said. “Removing the residual cortex after the lens has been put in and getting into the sulcus of the bag as well as 360 degrees around the posterior surface of the anterior capsule is a crucial step in modern refractive cataract surgery. This leaves less cortical material 360 degrees in the capsular bag. This reduces inflammation, asymmetric capsular contraction, IOP, and facilitates IOL exchange in the future.”
With bimanual I/A, Dr. Kandavel tries to make both ports directly across from each other to maximize the benefit. “I make the left-handed port where comfortable, and I make the right-handed secondary paracentesis directly across from it with consideration for LRIs if present first.”
With cortical cleanup, there’s a lot of advantages to being meticulous with the complete cleanup of every last visual fragment, Dr. Kandavel said, but it’s also important to go into the sulcus behind the iris to clean up. Many times, not only will you get access to cortex that you can’t see, but you’ll discover cortex that you were meaning to remove that’s now in the periphery of the bag without you even knowing, he said.
The advantages of that are theoretically, you reduce posterior capsular opacity formation, and that’s essential in refractive lens exchange because there are a lot of cases nowadays where physicians have to make a decision whether the multifocality of the lens or the optical features are causing certain aberrations in the early postop period, Dr. Kandavel said.
In today’s refractive cataract surgery world, surgeons have to be accustomed to offering lens exchange in certain cases. IOL exchange is made more facile by meticulous cortical cleanup because it’s the residual cortex that is a stimulant for capsular fibrosis, making the haptics easier to remove if that’s needed, Dr. Kandavel said. When cortical cleanup is not meticulous, there could be epithelial proliferation and the formation of Soemmerring’s rings, which are collections of large numbers of epithelial cells. They can cause decentration or late-term inflammation
Bimanual I/A is done through smaller incisions, Dr. Kandavel said, adding that he likes to use a reusable handpiece set by MST. It comes in multiple sizes (19-, 21-, and 22-gauge). The 22-gauge is what Dr. Kandavel uses to help with influx of irrigation. You can even use a different size irrigation handpiece and a smaller size aspiration handpiece if you prefer, he said. “The 22-gauge is approximately 700 microns, so I use a 1-mm sideport incision that’s a fixed thickness to create the two paracentesis ports,” he said. “By having a 1-mm sideport, the chamber stability is much better. You don’t get as much trampolining.” He added that chamber stability is greatly improved in bimanual I/A due to the smaller sideports, and the seal around those ports is considerably tighter, making for a more stable chamber. You do have to increase the bottle height, but because the irrigation is narrow, the effective pressure in the eye is not as high as the machine may indicate.
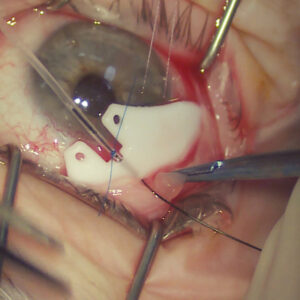
There are a number of other benefits to bimanual I/A, Dr. Kandavel said. “For instance, there are certain cases where we’ll encounter the need for a suture through the main incision. … Some surgeons use a nylon suture to secure the main incision when placing an accommodative lens. If you have to enlarge the incision, you can place and even tie the suture after placing the lens, and you can perform I/A through two sideports with the sealed main incision. You get good lens centration without as much fluctuation because you’re not coming in and out of a larger incision where the chamber may shallow and change the position of the lens; the chamber is rock solid, and you’ve hydrated your main incision or secured it with a suture. You’ve centered your lens, you come straight out of the eye, and the lens stays where you put it.”
There are certain cases where there are unstable chambers, like very long or very short eyes, and the facility of having a smaller irrigation handpiece and smaller incision gives the chamber a more solid feel, and it’s more versatile, he said.
Another example of an advantage of bimanual I/A, Dr. Kandavel said, is when you’re using it for MIGS procedures. You put in the lens and the MIGS device, and you want to prevent hypotony as much as possible directly after placing the MIGS device because you’ll get egress of blood through Schlemm’s canal and through the device. With bimanual I/A, you can increase the pressure, irrigate the blood out of the anterior chamber, keep the pressure a little higher, and limit the amount of blood in the AC. “I also find the smaller bimanual instruments particularly helpful for aspirating behind the IOL, which I perform in all cases, but especially in MIGS to prevent IOP spikes,” Dr. Kandavel said.
Bimanual I/A is also more zonule friendly, Dr. Kandavel said. Because you can get directly across and perpendicular to the cortex, you can strip tangentially and circumferentially to reduce zonular stress.
There’s also an advantage of bimanual I/A when you can use your secondary incision for other purposes, such as IOL manipulation for a toric lens or for centration, he said. CTR placement can be made easier, and you can use it for Malyugin ring removal because sometimes it’s advantageous to have a second approach to disengage one of the scrolls from the iris.
Dr. Ifantides agreed that bimanual I/A may be particularly helpful for more complex surgeries. It’s good for small pupils because if you have to sweep underneath the iris, you want something that is more elegant, he said. It’s smaller, and you can go underneath the iris and into the bag easier. “Additionally, sometimes with a small pupil, you need to use a second instrument to try to visualize the bag if you’re doing coaxial,” he said. “With this, you could use the irrigation portion of the bimanual to move the iris around a bit and visualize while you’re sweeping for cortex.”
Dr. Ifantides said bimanual I/A may also prove advantageous for special lenses that end up needing a larger wound. For example, when using the IC-8 Apthera (Bausch + Lomb) and needing to increase wound size, Dr. Ifantides has run into problems going back into the eye with coaxial and having a bigger wound than the sleeve allows for. You can get egress of fluid around the sleeve, which shallows the chamber, and the iris can come out if you’re not careful, he said. You can avoid that by using bimanual. “After you put in the lens, you have an enlarged wound, you can hydrate the main wound and switch to bimanual for the removal of the viscoelastic,” he said.
Types and tips
The biggest barrier is the additional cost. MST has a reusable product. Dr. Kandavel said he uses the same handpiece for years. There is a cost savings if you don’t have to pay for an additional irrigation handpiece, he said. In some cases, the handpiece is included with the phaco pack, but other times it’s a la carte, so it can be as much as $10–20 for the irrigation handpiece. It’s important with reusable bimanual I/A to have very good cleaning protocols because you can have residual cortex and potential TASS if everything is not cleaned correctly. You also want to be mindful if you’re using a reusable system that there are no barbs on the irrigation side.
“Alcon makes a coaxial handpiece that transforms into a bimanual handpiece, but unlike true bimanual handpieces, you don’t have to create that third incision,” Dr. Kandavel said. That allows the benefit of bimanual I/A without creating another incision. “The only disadvantage with that is that you have to put the infusion through the main incision, so the bimanual aspect of it only has the advantage of going through one sideport. It doesn’t necessarily give you the same access of having two sideports with true bimanual.”
Dr. Ifantides also uses a reusable bimanual I/A by MST. He added that Alcon makes a disposable polymer tip that can detach.
He said that for the paracentesis, it helps to make it slightly bigger than 1 mm so if you enlarge, you don’t stretch it out as much when maneuvering with bimanual, and it seals easier and isn’t leaky.
Dr. Ifantides also recommended speaking to “the people who support your machines and telling them that you’re interested in getting into bimanual because some settings can be adjusted to improve the performance.” He added, “the machine assumes you’re using coaxial, so if you switch to bimanual, you should adjust that.”
Additionally, Dr. Ifantides said that companies are usually good about sending trial sets if you’re interested in trying different products. That’s nice because you can do that before you pull the trigger, he said.
Article Sidebar
I wish I had …
Boris Malyugin, MD, PhD, Refractive Editorial Board member, shared what he wishes he had:
I am dreaming that the femtosecond laser IOL power adjustment technology will be available sooner rather than later. Although we do have the LAL (RxSight), using the femtosecond laser for that purpose seems to be more promising.
About the physicians
Cristos Ifantides, MD, MBA
Tyson Eye
Cape Coral, Florida
Rom Kandavel, MD
Colvard-Kandavel Eye Center
Encino, California
Relevant disclosures
Ifantides: Alcon, Bausch + Lomb, Johnson & Johnson Vision
Kandavel: Alcon, Glaukos
Contact
Ifantides: cristosmd@gmail.com
Kandavel: valleyeyedoctor@gmail.com