In Focus: Challenging Cataract Cases
September 2019
by Vanessa Caceres
EyeWorld Contributing Writer

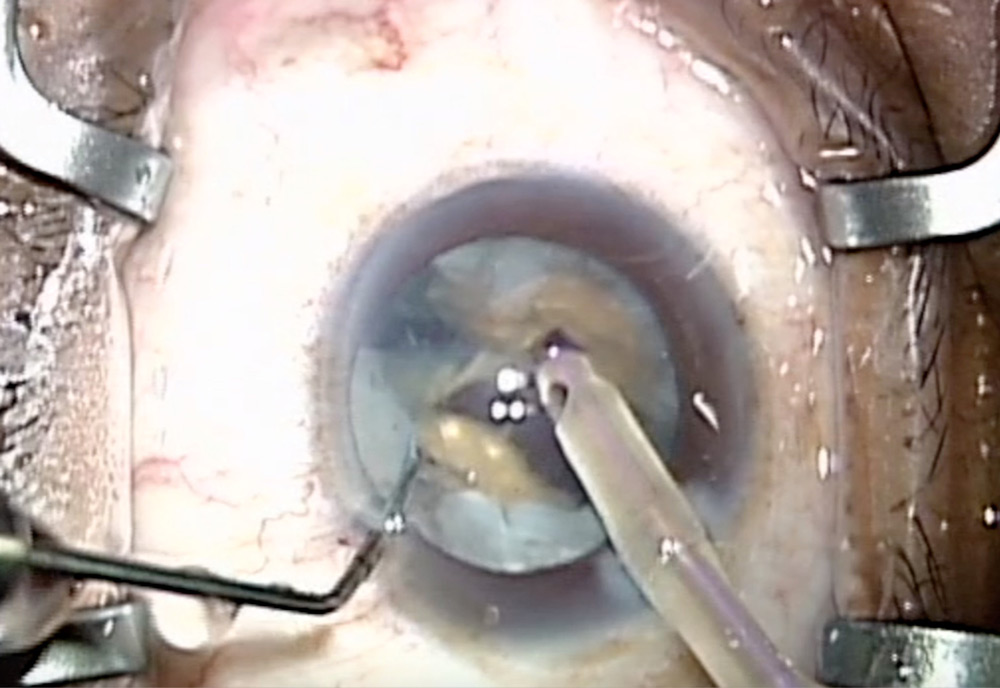
Source: Tal Raviv, MD
Dense white cataracts and mature brunescent cataracts can make surgery particularly challenging, yet the reward comes once patients can see again. “Patients with bilateral brunescent cataracts are typically at hand motions and are the happiest of patients [after surgery]. They go from being unable to live alone to being able to drive,” said Zaina Al-Mohtaseb, MD.
EyeWorld spoke with several seasoned surgeons to find out how they manage these types of cataracts.
Mature brunescent cataracts
A higher risk of complications and difficult visualization are two challenges associated with mature brunescent cataracts. Mature cataracts can be dark brown, red, white (with or without a liquid component), or black, said Johnny Gayton, MD.
“Many of the mature cataracts have a leathery plate at the bottom that makes cracking difficult,” Dr. Al-Mohtaseb said. “In addition, there is very little cortex and thus less protection of the posterior capsule.”
Trypan blue can help to visualize the capsule, which is often hard to see, and a deep phaco groove allows for a quicker procedure, said Doug Katsev, MD.
Use of a femtosecond laser with mature brunescent cataracts is potentially helpful to soften the lens nucleus and results in less ultrasound energy use for lens removal, Dr. Al-Mohtaseb said.
Dr. Katsev said that the femto laser can help in using less energy, but he does not think its use is a must.
One device that some surgeons have found helpful is the miLOOP (Carl Zeiss Meditec), which provides energy-free lens fragmentation. This is especially helpful for cataracts with a dense, leathery plate, Dr. Al-Mohtaseb said. “It helps crack the lens, which is one of the hardest parts in phacoemulsifying these dense cases. There is a short learning curve and the device is very helpful,” she said. She recommended practicing with the miLOOP first on less dense cases so that it can be visualized.
Dr. Gayton said to proceed with caution when using the miLOOP in dense cases with little to no cortex. “You can perforate or tear the capsule and/or disinsert zonules,” he said.
For nuclear disassembly of a mature brunescent case, make a deep groove, and be sure to hydrodissect to allow the lens to split easily, Dr. Katsev advised.
Dr. Al-Mohtaseb shared four pearls for nuclear disassembly:
- Widen the initial groove when sculpting.
- Use the stop-and-chop technique to decrease ultrasound energy usage
- Use the Nagahara phaco chopper to chop the lens into small pieces as much as possible, then use phaco to remove the pieces.
- Phaco in the capsular bag as much as possible.
Dr. Gayton added that the capsular opening is key. “Take as much time as you need to get a good result for the patient,” he said.
Source: Zaina Al-Mohtaseb, MD

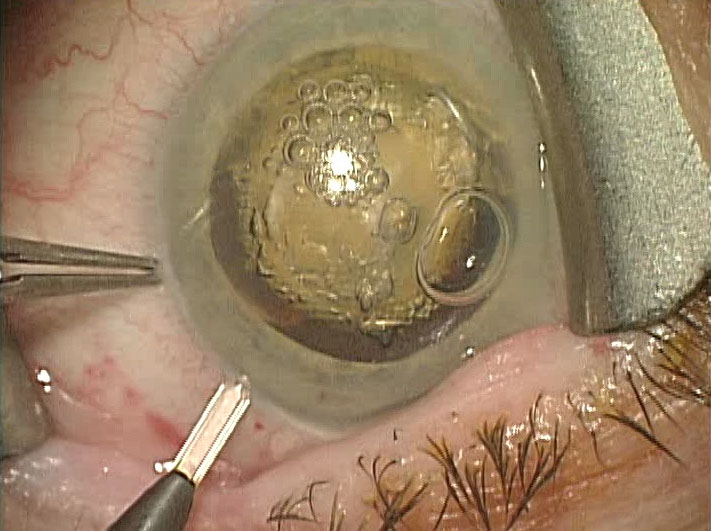
Source: Tal Raviv, MD
Dense white cataracts
Dense white cataracts are unpredictable, and surgeons often do not know what is causing them to be white. “When you approach a white cataract, be ready for anything,” said Paul Kang, MD. “If you can get [details] from the patient history or by looking at the cataract, it can help. Oftentimes, it’s not possible.”
Source: Johnny Gayton, MD
Denise Visco, MD, likens a dense white cataract to driving in a blizzard. “Eventually, as you begin working, everything gets kind of white, and you don’t have good contrast between the capsule and lens,” she said.
“White cataracts can either behave like any other cataract or they can have increased intraocular pressure with a high risk of anterior capsule tear out—the dreaded Argentinian flag sign,” said Tal Raviv, MD.
To help better manage these challenging cataracts and avoid additional surgical surprises, the surgeons shared a few suggestions:
- Create a good incision at the beginning that will not leak during the case. “It all starts with a good incision,” Dr. Visco said. “If you’re burping out viscoelastic or have poor chamber stability, it’ll make things more difficult.”
- Make sure the patient is dilated widely. Dr. Kang will use epi-Shugarcaine to help with the view.
- Stain the capsule with trypan blue. “If there’s not a good red reflex, it’s difficult if not impossible to see without some stain,” Dr. Kang said.
- Be mindful of your choices for an ophthalmic viscosurgical device (OVD). Dr. Kang uses a combination of Viscoat (sodium chondroitin sulfate/sodium hyaluronate, Alcon) on the endothelium along with Healon5 (sodium hyaluronate, Johnson & Johnson Vision) or a similar OVD. “In this case, I’m using Viscoat because I’m anticipating the cataract may be a little denser, and I want to protect the endothelium. I’m also anticipating the lens might be under pressure, which is why I’ll want to use a viscoelastic with a higher molecular weight so it won’t readily escape the anterior chamber,” he said.
- Keep the chamber pressurized, and release pressure if needed in a controlled manner. During that time, you often can find out if the cataract is rock hard or soft, Dr. Kang said.
- If an advanced white cataract has capsular plaque, try to plan the capsulotomy around the plaques so they will not tear, Dr. Raviv recommended. “If they are extensive, curved microscissors will be necessary to complete the rhexis,” he said.
- Use a stop-and-chop technique to disassemble the nucleus, Dr. Kang said.
A femtosecond laser can potentially help with capsulorhexis creation as it’s quick, Dr. Visco said. However, surgeons should use whatever is most comfortable for them, be it manual or with the femto laser, she added.
“Femtosecond laser capsulotomy has helped with white cataracts, though it’s not foolproof,” Dr. Raviv said.
Another advantage with the laser is that you can obtain Scheimpflug or OCT imaging of the lens to see what is happening internally. If imaging shows that the chamber is shallow or the lens appears under pressure, Dr. Visco will adjust the laser parameters to perform the capsulotomy even faster, to help decrease the chance of an incomplete rhexis or a tear out. As Dr. Raviv concurred, “A slower [capsulotomy] will likely be incomplete, since as soon as the capsule is entered, liquified cortex exits, blocking the femto, moving the capsule, and still leaving a risk of radialization.”
“The challenge with a white cataract is if you’re using a femto laser, the energy for softening the lens won’t penetrate,” Dr. Kang said. The bottom line is: Keep the laser in mind as a tool, but don’t expect it to be your go-to for all dense white cataracts you treat. That said, it still could be helpful for astigmatism correction if needed, Dr. Kang said.
Dr. Visco recommends having intraocular scissors on hand for whichever approach you use, be it femtosecond or manual. These can help you adjust the course for a capsulotomy that has gone wrong with either approach.
Another pearl from Dr. Visco: Don’t assume what kind of IOL or astigmatism correction the patient wants just because they have a white cataract. Although many of these patients may not qualify for premium technology due to other diseases present, such as diabetes, she still has treated patients who have wanted a premium refractive result. “It’s our due diligence to make sure the patients know all their options,” she said.
About the doctors
Zaina Al-Mohtaseb, MD
Associate professor of ophthalmology
Baylor College of Medicine
Houston
Johnny Gayton, MD
Eyesight Associates
Warner Robins, Georgia
Paul Kang, MD
Assistant clinical professor
Department of Ophthalmology
Georgetown University
Washington, D.C.
Douglas Katsev, MD
Sansum Clinic Ophthalmology
Santa Barbara, California
Tal Raviv, MD
Eye Center of New York
New York
Denise Visco, MD
Medical director
Eyes of York
York, Pennsylvania
Relevant financial interests
Al-Mohtaseb: None
Gayton: None
Kang: None
Katsev: None
Raviv: None
Visco: None
Contact information
Al-Mohtaseb: zaina1225@gmail.com
Gayton: jlgayton9@gmail.com
Kang: pkang@edow.com
Katsev: katsev@aol.com
Raviv: tal.raviv.md@gmail.com
Visco: dvisco@eyesofyork.com


