Cataract
Spring 2025
by Liz Hillman
Editorial Co-Director
Corneal edema after cataract surgery, or any intraocular surgery, is expected to an extent. Saba Al-Hashimi, MD, said swelling even out to week 2 postop is typical for cataract surgery. But as postop recovery stretches to 1 month or beyond, questions start rolling through the surgeon’s mind, and they begin to treat the situation differently: Did I miss Fuchs dystrophy? Is this a Descemet’s separation? Was too much energy used? What’s next?

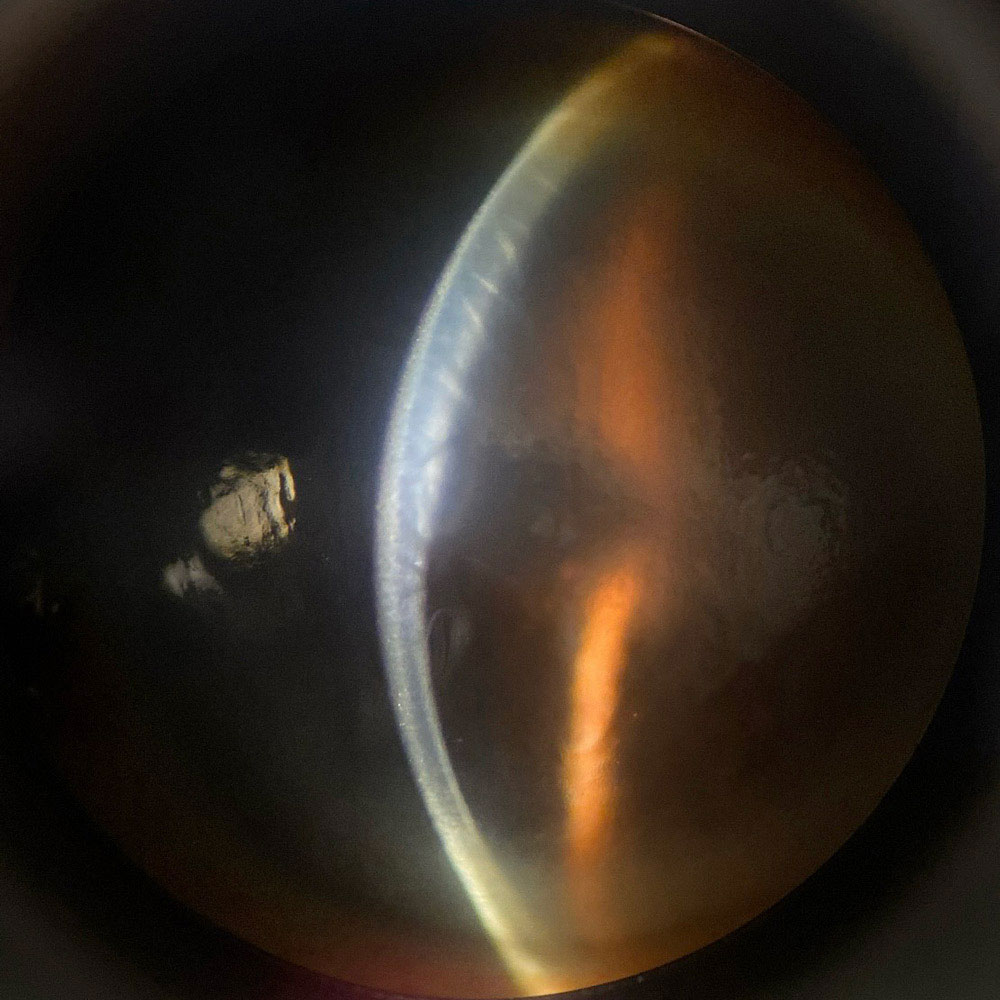
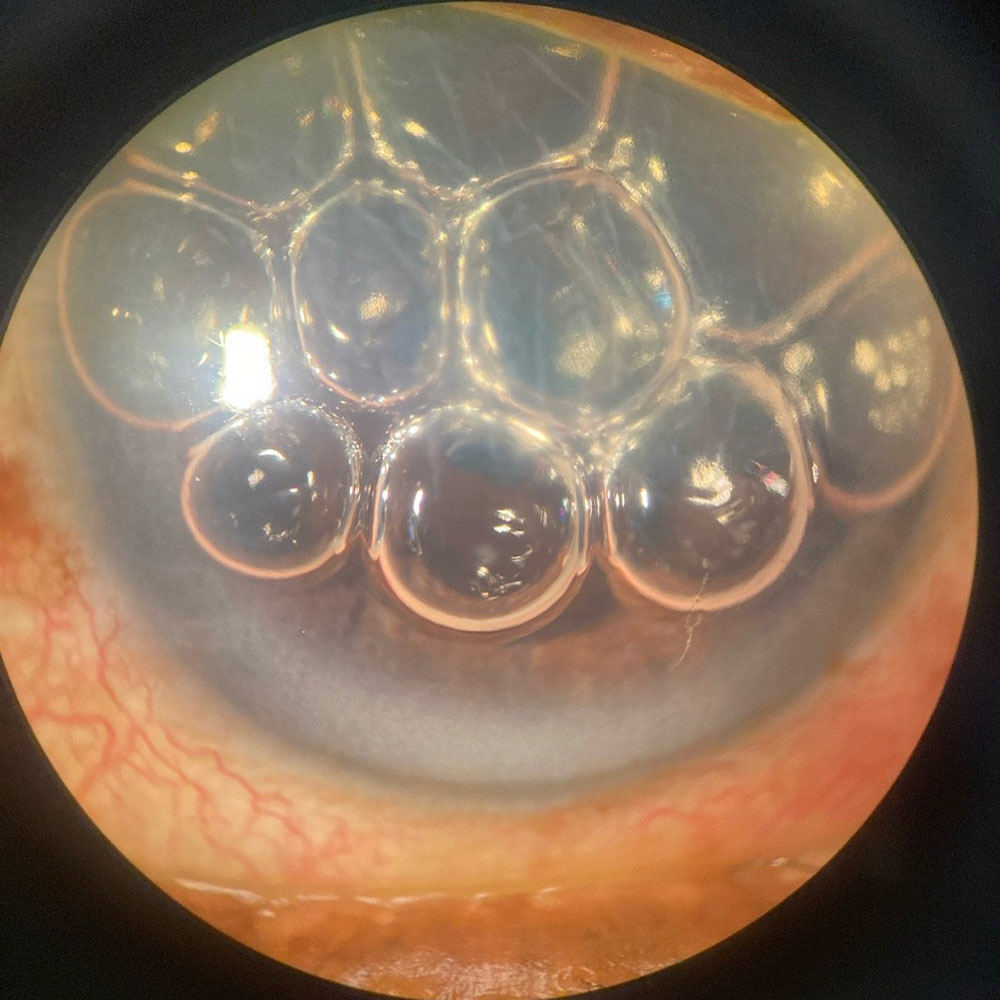
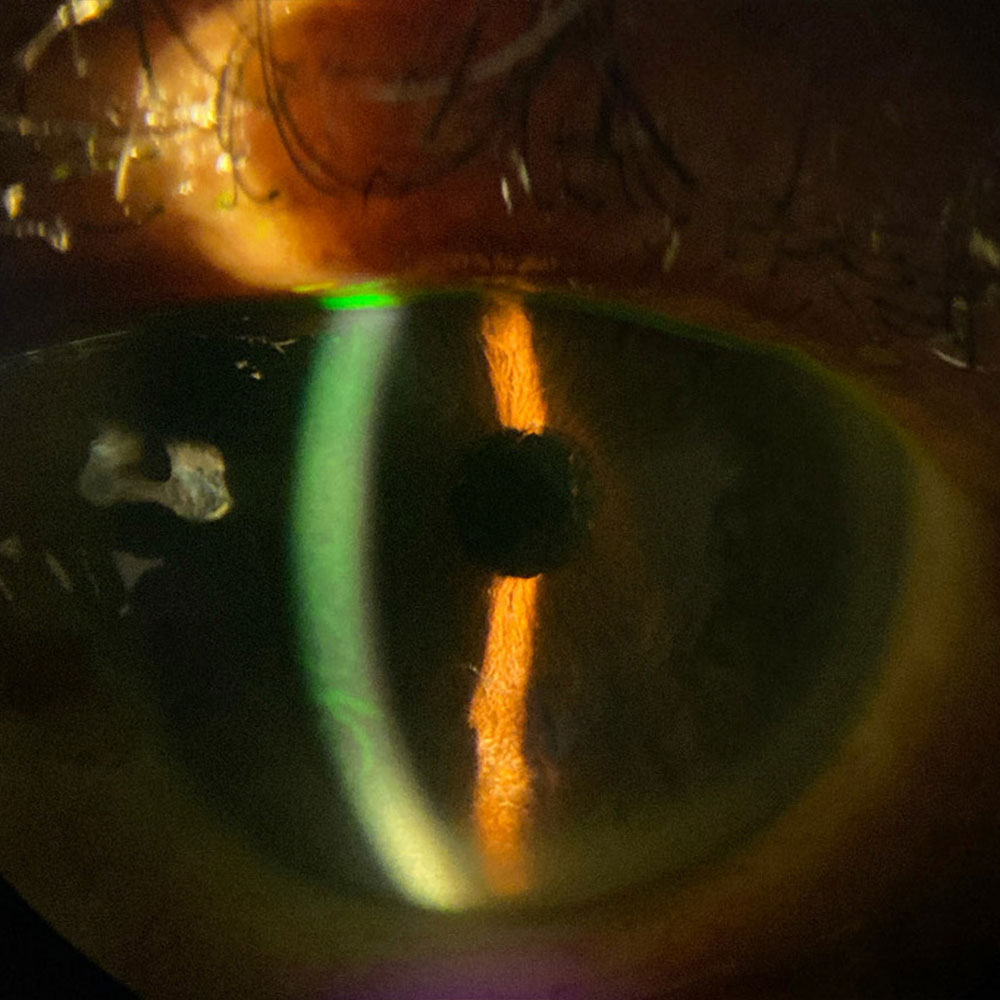
Source (all): Himani Goyal, MD
Preop contributors
There are several risk factors that put a patient at higher risk for prolonged corneal edema after cataract surgery. The most obvious, said Clara Chan, MD, is Fuchs dystrophy, with or without guttae. She also said any history of HSV could contribute as well.
“If patients have a known disease, we can counsel them: ‘There is a decrease in the health or number of endothelial cells in your cornea. These are the cells that pump out water from the cornea and help keep it clear. … We expect some corneal swelling normally, but you may have more because of this,’” said Himani Goyal, MD.
“Without regularly getting a specular microscopy preoperatively, this can easily be missed,” Dr. Al-Hashimi said of low endothelial counts that can be present without guttae. “If, however, the first eye ends up with more corneal edema than anticipated, it may be wise to obtain a specular microscopy before surgery on the second eye.”
Other risk factors, according to Dr. Chan, Dr. Al-Hashimi, and Dr. Goyal, include a dense arcus (which could put the patient at risk for retained nuclear fragments), small pupils (which might require expansion devices and more manipulation in the eye), dense cataracts (which could require more phaco energy), narrow angles, shorter anterior chamber depth (which puts you closer to the endothelium during surgery), and older age (which could make Descemet’s detachment more likely).
Dr. Goyal pointed out that patients with shallow chambers or endothelial disease might be more prone to iatrogenic Descemet’s tears. These tears, she said, are common in the area of the main wound. They often flap back up and are of no consequence, but if they occur, they can prolong edema.
Prevention
While you can’t change the anatomy of a small eye or dense lens, Dr. Al-Hashimi said some protective measures include use of a dispersive viscoelastic and keeping the phaco tip closer to the iris plane.
“Additionally, the use of a femtosecond laser can help fragment the nucleus, and chopping techniques can also be used to reduce the cumulative dissipated energy from the phaco tip, which can also reduce the chances of developing edema,” he said.
Overall tips Dr. Al-Hashimi provided were: with very dense cataracts, refill with OVD multiple times during the case (“the rule of thumb is to refill after each quadrant is removed”); aspirate some hyperthermic OVD over the cataract before using high phaco energy for sculpting; use care with wound construction to avoid a jagged internal main wound, which increases the risk for Descemet’s detachment; ensure sufficient flow using phaco machine settings, and don’t crimp the phaco needle sleeve; angle the phaco tip down and keep the eye parallel to the ground; take time out prior to IOL insertion to ensure it’s the right IOL; avoid PCR by not over-hydrating dense lenses; and hydrate wounds gently at a physiologic IOP to lower Descemet’s detachment risk.
“Longer operating times are associated with corneal edema. In cases where there is a complication or the cataract surgery is more complex, the chances of seeing corneal edema postoperatively are increased,” Dr. Al-Hashimi said. “Intraoperatively, using a dispersive viscoelastic (and replenishing as needed) can help protect the endothelium. If you see bubbles in the anterior chamber that are freely mobile instead of fixed in place, it can be a sign that the dispersive viscoelastic you used may no longer be adequately present in the eye; this is a good signal to stop and replenish if the patient has risk factors for developing edema.”
In smaller chambers, Dr. Goyal said to consider doing a pars plana vitrectomy to help deepen the chamber if you are comfortable with this technique, or use preop mannitol to shrink the vitreous. “Part of the reason pseudophakic bullous keratopathy has become less common is that our phaco machines and surgical techniques have become more efficient, making our surgeries shorter and requiring less energy. One important advancement in our phaco machines is the ability to adjust the intraocular pressure at which we operate,” Dr. Goyal said. “Normally, I’m operating at physiologic eye pressure, but if I need to deepen the chamber, I can raise the IOP. There is potential to disturb the dispersive viscoelastic in the eye when operating at a higher IOP, however, as long as the irrigation ports are pointing sideways and the wound is sealed around the phaco sleeve, disturbance of the dispersive viscoelastic above you should be minimal.”
Dr. Goyal said she also thinks there is value in using a smaller than standard speculum for patients with deep-set or smaller eyes. Making the patient more comfortable can affect how long the surgery takes and thus reduce the risk for an increase in postop edema. “Giving patients a little more anesthesia to keep them relaxed and from squeezing or baring down can affect the surgery,” she said.
Diagnosis
Dr. Chan said anterior segment OCT is helpful to diagnose a Descemet’s membrane detachment or retained lens fragment as the cause for prolonged corneal edema. Dr. Al-Hashimi said pachymetry can confirm the diagnosis of prolonged corneal edema, but he added that it’s important to keep TASS in the differential if the edema is significant and there is a high degree of intraocular inflammation in the anterior chamber early on.
Dr. Goyal said corneal edema is obvious when you see Descemet’s folds associated with clouding of the stroma, but once the Descemet’s folds resolve, reviewing the preop measurements and history and comparing to postop topography or pachymetry can help determine if there is persistent edema.
Treatment
Once it’s clear the edema is not resolving, Dr. Al-Hashimi said the first thing is “don’t panic.”
“Not uncommonly, corneal edema will resolve with time. Using a more frequent topical steroid regimen may help speed up recovery. It can take several weeks before corneal edema fully resolves,” he said. “It is best to follow patients with serial pachymetry to ensure the thickness continues to trend downward. This gives patients confidence that their situation is improving objectively even if their vision does not seem to be improving at first. If after 4 weeks you are no longer seeing progress, there is a high probability the patient will ultimately need an endothelial keratoplasty to resolve the issue. Sodium chloride ophthalmic solution drops or ointment can be used to help speed up recovery, but this typically is only useful when there is epithelial edema.”
Dr. Chan said treatment of the edema depends on its etiology and whether there was any pre-existing endothelial compromise or disease present.
“If a retained nuclear cataract piece is removed within a week to a month, the cornea, if otherwise healthy, can typically clear up in 1–4 weeks,” she said. “If a Descemet’s membrane detachment is rebubbled within 1–3 weeks, [it] can usually have a clear cornea within a similar timeframe. Beyond a month the Descemet’s membrane usually becomes fibrosed and can no longer contour against the stroma properly, and a DMEK may be needed. A history of HSV endothelial disease and/or iritis may also cause the endothelial cells to be dysfunctional or deficient, leading to a greater risk of prolonged corneal edema after cataract surgery, especially if other intraoperative risk factors are not mitigated.”
Dr. Goyal said when there is no improvement of corneal edema or persistent edema at postop month 1, it’s time to intervene. She starts treatment with sodium chloride drops or ointment. If this does not help, she would consider a rho-kinase (ROCK) inhibitor, which she said “can help our endothelial cells function at their best and are low risk.” If a ROCK inhibitor is going to help, it would improve within a few days to weeks. If after that there is insufficient improvement, Dr. Goyal said it’s time to consider an endothelial keratoplasty (DMEK), though she hopes in a few years endothelial cell therapy could be an option.
If there is long-standing corneal edema, especially in the setting of bullae and microcystic edema, Dr. Al-Hashimi said subepithelial scarring could develop, limiting vision even after a successful endothelial keratoplasty. “It is best to try addressing corneal edema with additional surgery within a few months to minimize permanent scarring,” he said. Dr. Chan said patients could suffer pain from ruptured bullae or foreign body sensation from microcystic corneal edema that can occur with prolonged corneal edema.
Dr. Chan said surgeons should carefully examine for post-cataract surgery corneal edema. Always consider a Descemet’s membrane detachment or retained nucleus piece as well because managing these problems as soon as possible can successfully reverse postoperative corneal edema.
About the physicians
Saba Al-Hashimi, MD
Associate Professor of Ophthalmology
University of California, Los Angeles
Los Angeles, California
Clara Chan, MD
Associate Professor of Ophthalmology
University of Toronto
Toronto, Canada
Himani Goyal, MD
Clinical Associate Professor
NYU Langone Health
New York, New York
Relevant disclosures
Al-Hashimi: None
Chan: Théa
Goyal: Alcon
Contact
Al-Hashimi: alhashimi@jsei.ucla.edu
Chan: clarachanmd@gmail.com
Goyal: himani.goyal.md@gmail.com


