Glaucoma: YES Connect
Summer 2025
by Ellen Stodola
Editorial Co-Director
An emphasis on sustainability in healthcare has gained momentum in recent years. Enhancing patient care through improving cost efficiency, reducing waste, and minimizing environmental impact have become growing priorities in glaucoma and other ophthalmic subspecialties. As the global burden of glaucoma continues to rise, it is essential to adopt practices that balance effective treatment with responsible resource utilization. Traditional glaucoma surgeries often involve disposable instruments and medical supplies that generate waste and environmental harm. By adopting more sustainable practices, we can reduce cost and ecological footprint while maintaining high-quality care.
Economically, sustainability also plays a crucial role. With the rising costs of medical care and the need for ongoing treatments, utilizing durable equipment, reusable instrumentation, and streamlining resource use can lower long-term healthcare expenses. Additionally, sustainable approaches to glaucoma surgery can make treatment more accessible to underserved populations, improving equity in healthcare delivery.
We are fortunate to have a group of glaucoma specialists who are experts in sustainability offer us their perspective on how to make meaningful changes to your own clinical practice.
Shivani Kamat, MD, YES Connect Guest Editor
The efficient use of resources and cutting down on waste have become popular topics across all of medicine. Many physicians are becoming conscious of the number of resources used and thinking about ways to be more sustainable, while still ensuring safe and successful procedures for patients. In this issue’s YES Connect column, several physicians discussed sustainability in ophthalmology, particularly the glaucoma subspecialty.
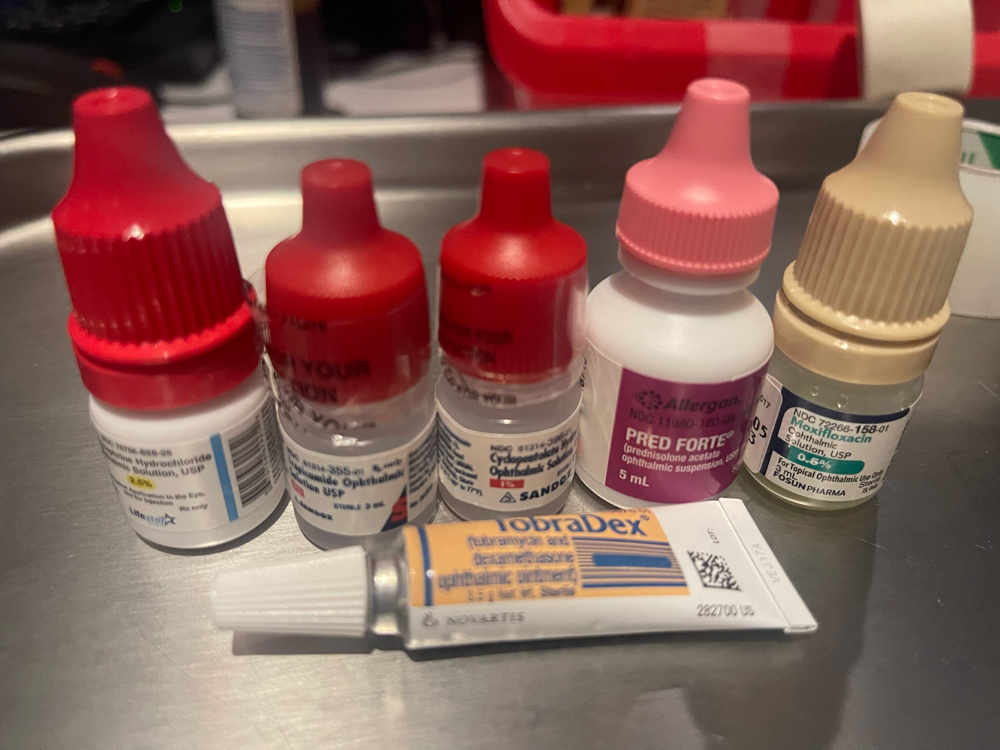
Source: Aakriti Garg Shukla, MD, MSc
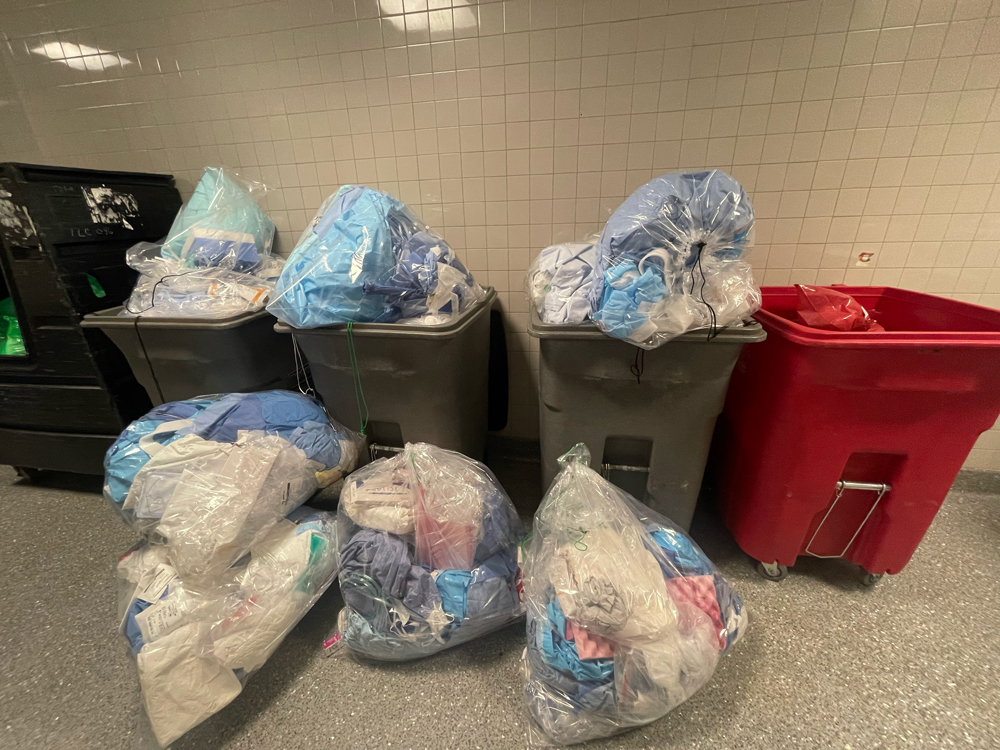
Source: Aakriti Garg Shukla, MD, MSc
Concerns with sustainability in glaucoma
One of physicians’ main goals, said Alan L. Robin, MD, is we never want to do harm, but we also don’t want to be wasteful, from a financial perspective and an environmental perspective, which can be equally harmful. Paying attention to sustainability might be a new mindset for some physicians, as it’s not something that’s taught in training but is something that’s been gaining ground recently.
Samantha Goldburg, MD, Lucy Li, MD, Aakriti Garg Shukla, MD, MSc, Mary Qiu, MD, and Emily Schehlein, MD, recently researched the topic of sustainability in glaucoma together. They noted that there are several concerns, and they broke these down into issues related to surgery, clinic, pharmaceutical waste, and transportation.
In the operating room, Western surgical facilities typically have single-use surgical equipment, excessive draping, large packaging of materials, paper instructions for surgical devices, lack of recyclable material, and lack of recycling bins in the operating rooms, they said. Examples of items that are only used once in cataract surgery in the U.S. and other Western nations include balanced salt solution bags, OVDs, I/A tips and sleeves, phaco tips and sleeves, cassettes, tubing, cannulas, and syringes.
Dr. Robin noted the package inserts included with IOLs, viscoelastics, MIGS devices, and many other products. They are rarely read and may be out of date by the time they are read. Although not too large, considering that more than 31 million cataract surgeries are done annually, the amount of paper wasted is astounding, he said. An electronic option or QR code would not only minimize waste but keep the information current when referenced.
Disposable instruments, drapes, and gowns are a source for waste, and sterilizing these and reusing them could substantially minimize waste.
Drs. Goldburg, Li, Shukla, Qiu, and Schehlein noted that the Aravind Eye Care System (AECS) in India reuses all these items for multiple patients without sterilization, except for the instruments that contact a patient’s eye, which undergo IUSS without wrapping of surgical instruments.1 “AECS was found to have a POE [postoperative endophthalmitis] rate of 0.04% in 2 million cases using their standard protocols,2 which is identical to the AAO’s reported rate of POE in the U.S.3 The POE rate in the AECS dropped further to 0.01% with adoption of routine intracameral moxifloxacin while maintaining their prior protocols.”4
Dr. Robin said that he began to question ways to be more sustainable, and he used the Aravind Eye Hospital as an example of being conscious about sustainability. They have lower complication rates in cataract surgery than we do in the U.S., he said. “We’ve learned that they recycle everything that they can, and they even divide plastics into those that can be sold to others versus plastics that they can recycle.”
In the clinic, single-use equipment has become the mainstay given the theoretical risk of disease transmission, Drs. Goldburg, Li, Shukla, Qiu, and Schehlein said. However, there are clear AAO and CDC guidelines stating that reusable tonometry tips can be sufficiently disinfected with 5,000 parts per million sodium hypochlorite.5
Dr. Robin noted glaucoma drops as an area where physicians can seek to become more sustainable. We often use drops for one day or one patient, then they are thrown away, he said. This is an issue in both glaucoma and cataract surgeries in the preop and postop periods. He mentioned that some patients have trouble putting drops in their own eyes and often contaminate the drops. In operating rooms, however, it’s a nurse or a technician putting drops in the eyes, so the products are not contaminated, and Dr. Robin said it doesn’t make sense to be wasteful with these.
The worst part is they’re thrown in a trash can, which is put into our landfill, and there is a large chance that the pharmaceuticals eventually land in our drinking water. “I’m really concerned about that,” Dr. Robin said.
In a 2019 study of four surgical centers, almost 50% of all drugs and two-thirds of topical drugs were discarded after a single use during phacoemulsification surgery, Drs. Goldburg, Li, Shukla, Qiu, and Schehlein noted, adding that the authors estimated that this drug waste generated 23,000 to 105,000 metric tons of unnecessary CO2eq emissions annually in the U.S.6
Additionally, transportation to and from the ophthalmology clinic and OR has been shown to be the greatest source of carbon emissions related to ophthalmic care.7 Most emissions come from transportation in cars. This is particularly concerning for glaucoma patients who require frequent follow-up, they said.
“The number of people affected by glaucoma worldwide continues to increase and is estimated to be nearly 112 million by 2040.8 As glaucoma prevalence rises, there will be a growing number of people who require timely diagnosis and management of this potentially blinding condition. Resources essential to providing this care will further challenge already stretched healthcare systems and will contribute to the impending climate crisis,” they said.
Different procedures and practices contribute waste in different ways. In Western operating rooms, almost every piece of equipment is single use and gets thrown away at the end of the case, Drs. Goldburg, Li, Shukla, Qiu, and Schehlein said. In a British study, one phacoemulsification procedure in the U.K. was found to generate about 130 kg carbon dioxide equivalent, which is the same as driving a car 310 miles. For reference, an estimated 5.2 million cataract surgeries were performed in 2017 in the U.S., and this rate is expected to grow 72% by the year 2036.9
Procurement of pharmaceuticals is a large contributor to overall surgical emissions, and several glaucoma surgeries require the use of pharmaceuticals, such as MMC or 5-FU. Disposal of pharmaceuticals additionally contributes to the carbon footprint, as it requires incineration, which releases greenhouse gases, leading to trapped heat and contributing to global warming. Single use of large eye drop bottles similarly contributes significantly to waste in the operating room setting.
Another area where Dr. Robin sees waste is having an anesthesiologist for every surgery. Most patients are cooperative, healthy, and have minimal risks of systemic adverse events. Additionally, there are risks to over sedating patients. Almost all patients who are healthy don’t necessarily require an anesthesiologist, he said.
Dr. Robin also noted water use during ophthalmological surgery as an area that could be improved. “I think all of us have learned to use scrubs that are based on water and either betadine or chlorhexidine before we start the day and in between all cases; a lot of glaucoma surgeons can do 10–15 cases, if not more, a day.” He noted that alcohol-based scrubs, which are chlorhexidine alcohol, betadine scrubs are less wasteful of natural resources. He added that in many parts of the countries like California and Arizona, there is a shortage of water. CDC guidelines say that you can use either alcohol-based scrubs or water, and he suggested that an emphasis in training would help implement this in more areas.
More sustainable practices in the OR and clinic
To be able to implement new practices focused on sustainability, Dr. Robin said this would require data, adding that we need to reexamine the whole system. We need to figure out which steps are actually needed and eliminate unnecessary steps. To implement change, Dr. Robin said it will be important to involve industry as well. You need to balance profit and the need for change, and many companies have been supportive so far.
Drs. Goldburg, Li, Shukla, Qiu, and Schehlein said that in patients with open angle glaucoma, there is often a discussion regarding whether the patient should start treatment with drops or selective laser trabeculoplasty (SLT). Laser procedures may be a more sustainable way to treat glaucoma patients than alternative options. The energy used for SLT has been found to be negligible in terms of carbon emissions. Moreover, bilateral laser procedures should be performed, when possible, to decrease the amount of patient transportation. “In the clinic, reusable tonometry tips and gonioprisms should be used and disinfected properly rather than single-use items. Our goal should be to properly disinfect multiuse items to prevent patient infection while reducing the carbon footprint of our practice.”
Procedures such as suture gonioscopy-assisted transluminal trabeculotomy and bent ab interno needle goniectomy may be preferable to other MIGS from a carbon footprint standpoint, as they use readily available equipment in the OR and avoid waste from excessively large packaging and procurement of new devices. “In addition, autologous patch grafts such as scleral lamellar grafts or autologous capsular patch grafts may be considered to avoid the use of pre-made grafts that come in large, wasteful packages and require separate procurement,” they said.
Drs. Goldburg, Li, Shukla, Qiu, and Schehlein noted that early intervention in glaucoma may help to lessen the carbon footprint of care because it may decrease the number of follow-up visits associated with perioperative care if the patient were to require a surgery such as a trabeculectomy.
“One strategy to help address sustainability in the care of glaucoma patients is to incorporate more telehealth into our practice,” they said. “Several studies have shown high adherence rates and patient satisfaction associated with virtual glaucoma appointments.10,11 Virtual visits are most successful when done by glaucoma specialists and if moderate-to-severe or unstable glaucoma patients are excluded.”12 They also noted that there are a few visual field devices that can be used at home, including exams on a tablet,13 a head mounted display,14 a PC monitor, or virtual reality glasses.15 There are also tonometers that patients can use at home, including the iCare HOME2; patients’ IOP readings have been shown to correlate well with Goldmann applanation.16
About the physicians
Samantha Goldburg, MD
PGY-4 Ophthalmology Resident
Zucker School of Medicine at Hofstra/Northwell
Hempstead, New York
Lucy Li, MD
PGY-4 Ophthalmology Resident
New York Medical College
Westchester Medical Center
Valhalla, New York
Mary Qiu, MD
Glaucoma Specialist
Department of Ophthalmology and Visual Science
University of Chicago
Chicago, Illinois
Alan L. Robin, MD
Emeritus Associate Professor of Ophthalmology and International Health
Johns Hopkins University
Baltimore, Maryland
Emily Schehlein, MD
Glaucoma Specialist
Brighton Vision Center
Brighton, Michigan
Aakriti Garg Shukla, MD, MSc
Glaucoma Specialist
Leonard A. Lauder Associate Professor of Ophthalmology
Columbia University Medical Center
New York, New York
References
- Ravindran RD, et al. Incidence of post-cataract endophthalmitis at Aravind Eye Hospital: outcomes of more than 42,000 consecutive cases using standardized sterilization and prophylaxis protocols. J Cataract Refract Surg. 2009;35:629–636.
- Shukla AG, et al. Reusing surgical materials for cataract surgery: an assessment of potential contamination. J Cataract Refract Surg. 2024;50:993–999.
- Pershing S, et al. Endophthalmitis after cataract surgery in the United States: a report from the Intelligent Research in Sight Registry, 2013–2017. Ophthalmology. 2020;127:151–158.
- Haripriya A, et al. Endophthalmitis reduction with intracameral moxifloxacin prophylaxis: analysis of 600,000 surgeries. Ophthalmology. 2017;124:768–775.
- Schehlein EM, Robin AL. Should we use disposable tonometers and gonioprisms in the office? Ophthalmol Glaucoma. 2025;8:109–111.
- Tauber J, et al. Quantification of the cost and potential environmental effects of unused pharmaceutical products in cataract surgery. JAMA Ophthalmol. 2019;137:1156–1163.
- Foo K, et al. The carbon footprint of glaucoma care with drops or laser first. Clin Exp Ophthalmol. 2025;53:435–437.
- Tham YC, et al. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121:2081–2090.
- Miller KM, et al. Cataract in the Adult Eye Preferred Practice Pattern. Ophthalmology. 2022;129:P1–P126.
- Lozano AC, et al. Telemedicine for screening and follow-up of glaucoma: a descriptive study. Telemed J E Health. 2024;30:1901–1908.
- Nikita E, et al. Expansion of patient eligibility for virtual glaucoma clinics: a long-term strategy to increase the capacity of high-quality glaucoma care. Br J Ophthalmol. 2023;107:43–48.
- Mercer R, Alaghband P. The value of virtual glaucoma clinics: a review. Eye (Lond). 2024;38:1840–1844.
- Prea SM, et al. Uptake, persistence, and performance of weekly home monitoring of visual field in a large cohort of patients with glaucoma. Am J Ophthalmol. 2021;223:286–295.
- Alawa KA, et al. Low-cost, smartphone-based frequency doubling technology visual field testing using a head-mounted display. Br J Ophthalmol. 2021;105:440–444.
- Tsapakis S, et al. Home-based visual field test for glaucoma screening comparison with Humphrey perimeter. Clin Ophthalmol. 2018;12:2597–2606.
- Mudie LI, et al. The Icare HOME (TA022) Study: performance of an intraocular pressure measuring device for self-tonometry by glaucoma patients. Ophthalmology. 2016;123:1675–1684.
Relevant disclosures
Goldburg: None
Li: None
Qiu: None
Robin: None
Schehlein: None
Shukla: None
Contact
Goldburg: samantha.goldburg@gmail.com
Li: lucysfmatch@gmail.com
Qiu: mary.qiu@gmail.com
Robin: arobin@glaucomaexpert.com
Schehlein: emschehlein@gmail.com
Shukla: ag2965@cumc.columbia.edu


