Cornea
April 2023
by Liz Hillman
Editorial Co-Director
Last year, an EyeWorld article took a look at the status of trabeculectomy in glaucoma practice; while it still has a place in the glaucoma treatment paradigm, according to some, it is being taught less and less in training programs in favor of newer therapies. Is the same occurring with DSAEK?

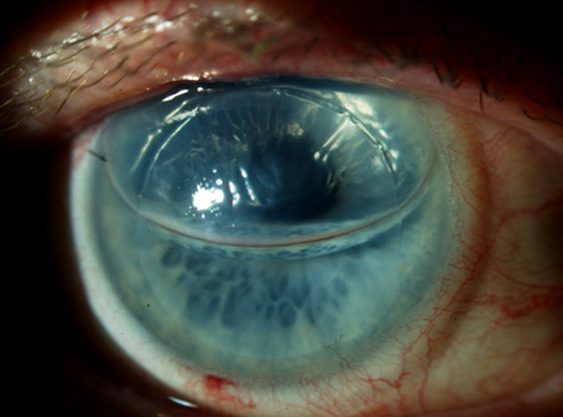
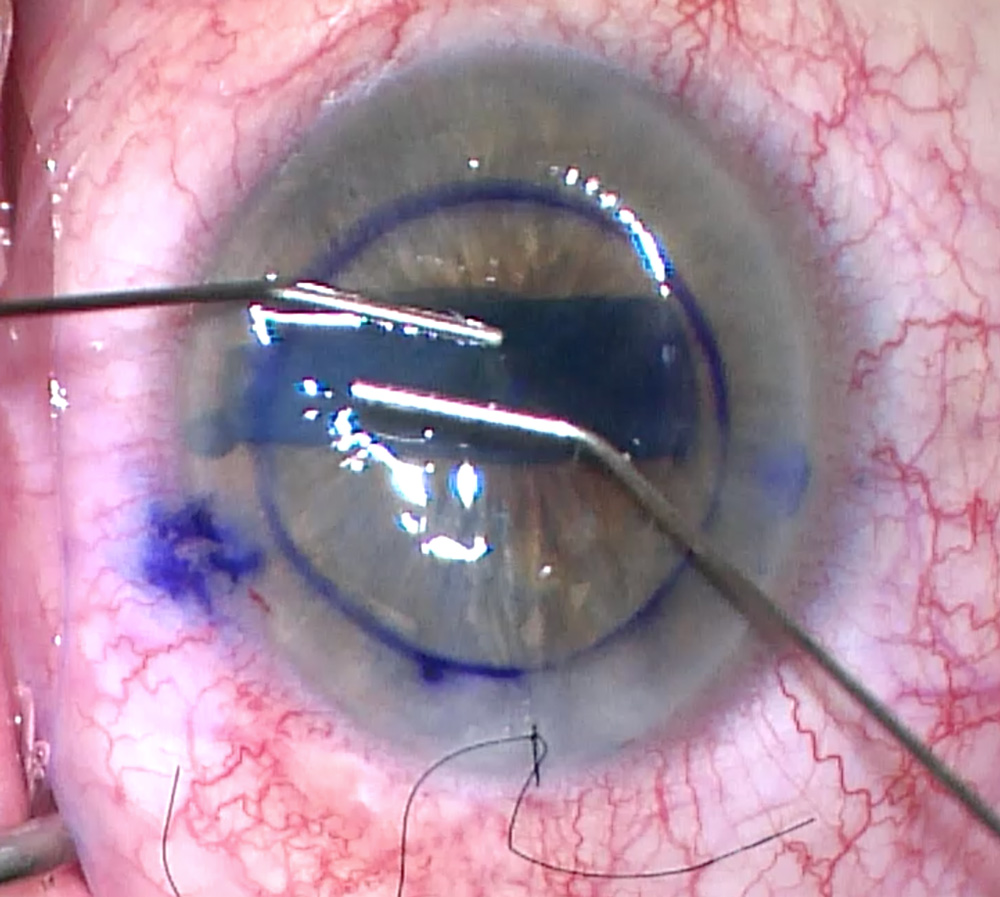
Source: Clara Chan, MD
Nandini Venkateswaran, MD, and Winston Chamberlain, MD, PhD, both said they had DSAEK training (DMEK wasn’t even a thing when Dr. Chamberlain was in residency or fellowship, he said) and think there continues to be a place for it, even while DMEK has gained increasing popularity.
Dr. Chamberlain thinks surgeons in training are likely still getting enough DSAEK exposure.
“Most surgeons who perform endothelial keratoplasty are still doing both surgeries, and training centers are teaching these skills to residents and fellows,” he said. “Many residencies, including ours at the Casey Eye Institute, now expose residents to DMEK and DSAEK. Our second year residents assist in both types of procedures and perform a small number during their senior year. Still, a majority of this surgical training takes place during a cornea fellowship.
“Both surgeries are taught thoroughly with a variation of techniques to our fellows, but DSAEKs still tend to be skewed toward the more complicated eyes that have had prior vitrectomies, glaucoma surgeries, anterior chamber IOLs, or have abnormal iris anatomy,” Dr. Chamberlain continued. “The 2021 Eye Bank Association of America (EBAA) Statistical Report reflects that DMEK is rising and likely soon, within the next year or 2, will equal the number of DSAEKs and PKPs done in the U.S. So, the three types of surgery will almost be even in distribution. Currently, DMEK is the main choice for uncomplicated Fuchs dystrophy and bullous keratopathy. The EBAA Statistical Report showed that about 64% of keratoplasties in the U.S. in 2021 were DMEK or DSAEK, and 52% of DSAEK and DMEK done in the U.S. were done for endothelial dystrophy. The 52% is probably an underestimate given that some surgeons don’t accurately report indications for surgery, and some EKs are done to replace a failing graft that was previously done for Fuchs dystrophy.”

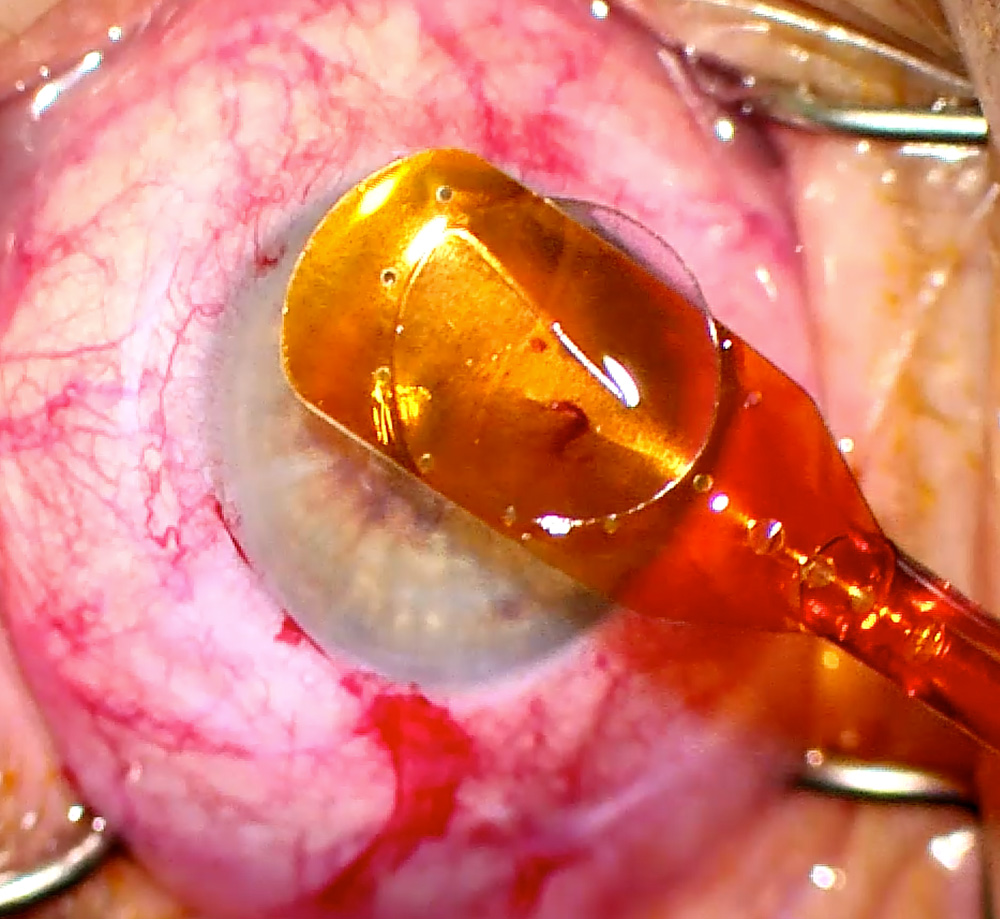
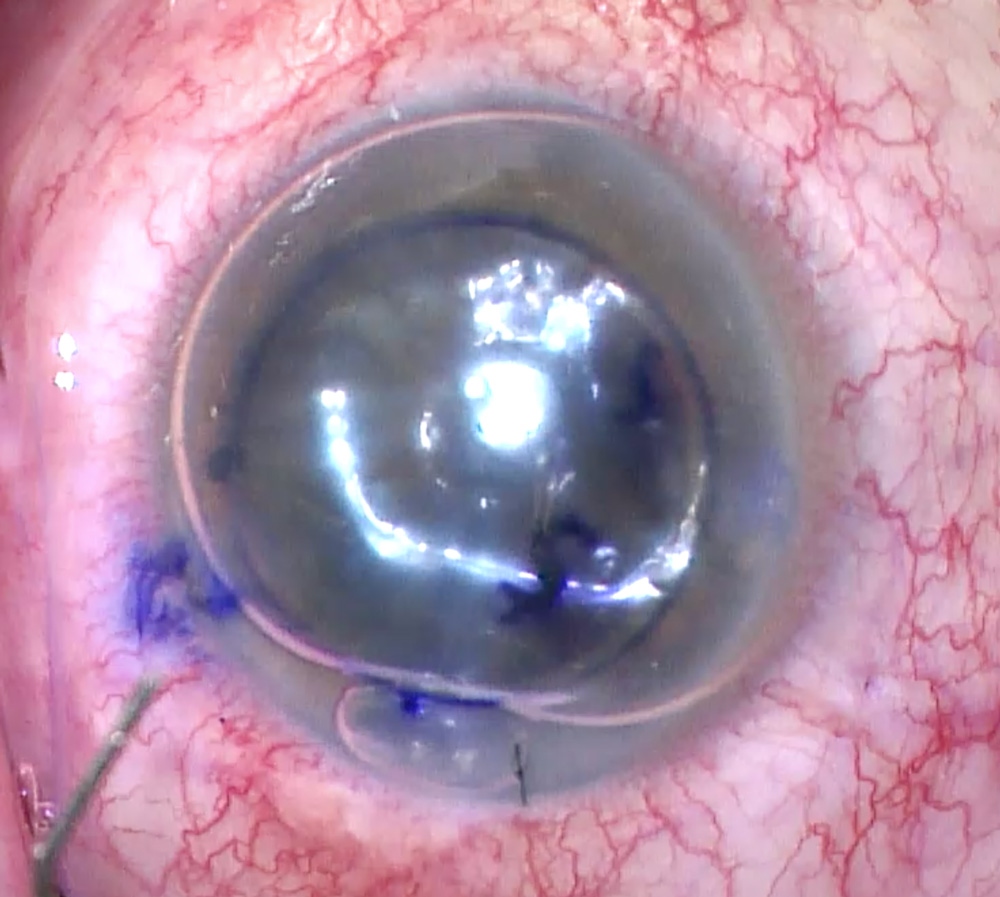
Source: Clara Chan, MD
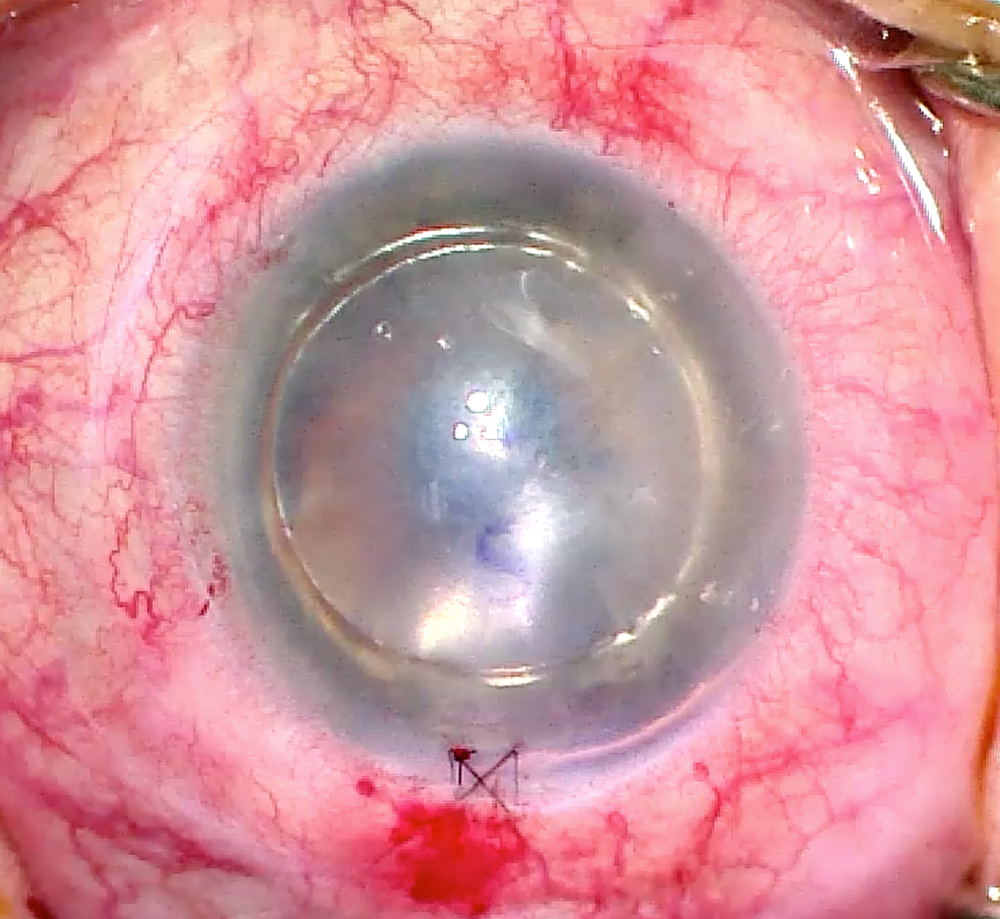
Source: Clara Chan, MD
Dr. Venkateswaran said experience with DMEK or DSAEK for those in training depends on the patient population they see and the technique with which attending ophthalmologists are more comfortable.
“If you have a clinic where you are predominately seeing patients with Fuchs dystrophy or pseudophakic bullous keratopathy in otherwise healthy eyes, I think the majority of cornea surgeons are trending toward performing DMEK. It’s the least invasive lamellar keratoplasty technique [and has] lower risks of rejection with improved vision outcomes compared to DSAEK. It’s an enjoyable surgical technique to learn and perform as well. But you can also have a cohort of eyes that aren’t going to necessarily shine with DMEK,” Dr. Venkateswaran said, noting that she did a lot of DSAEK in residency and a lot of DMEK in fellowship based on what surgical option was best for the patients she was caring for.
Dr. Venkateswaran and Dr. Chamberlain think there is still a place for DSAEK in cornea practice.
“DSAEK still has a solid role in corneal transplantation, and therefore techniques and training emphasis are important. One of the driving forces for DMEK is the result of two randomized controlled trials that demonstrated that DMEK outperformed ultrathin DSAEK in patients with Fuchs and bullous keratopathy in terms of vision at 1 year and recovery time.1 One of those trials showed DMEK still giving better visual acuity at 2 years after surgery than ultrathin DSAEK,2” Dr. Chamberlain said. He noted, however, that the trials focused on less complicated eyes. “There are fewer high-standard publications rigorously assessing DMEK’s long-term performance in more complicated eyes. These eyes create surgical challenges for successfully completing DMEK, and therefore DSAEK may still be the best approach.”
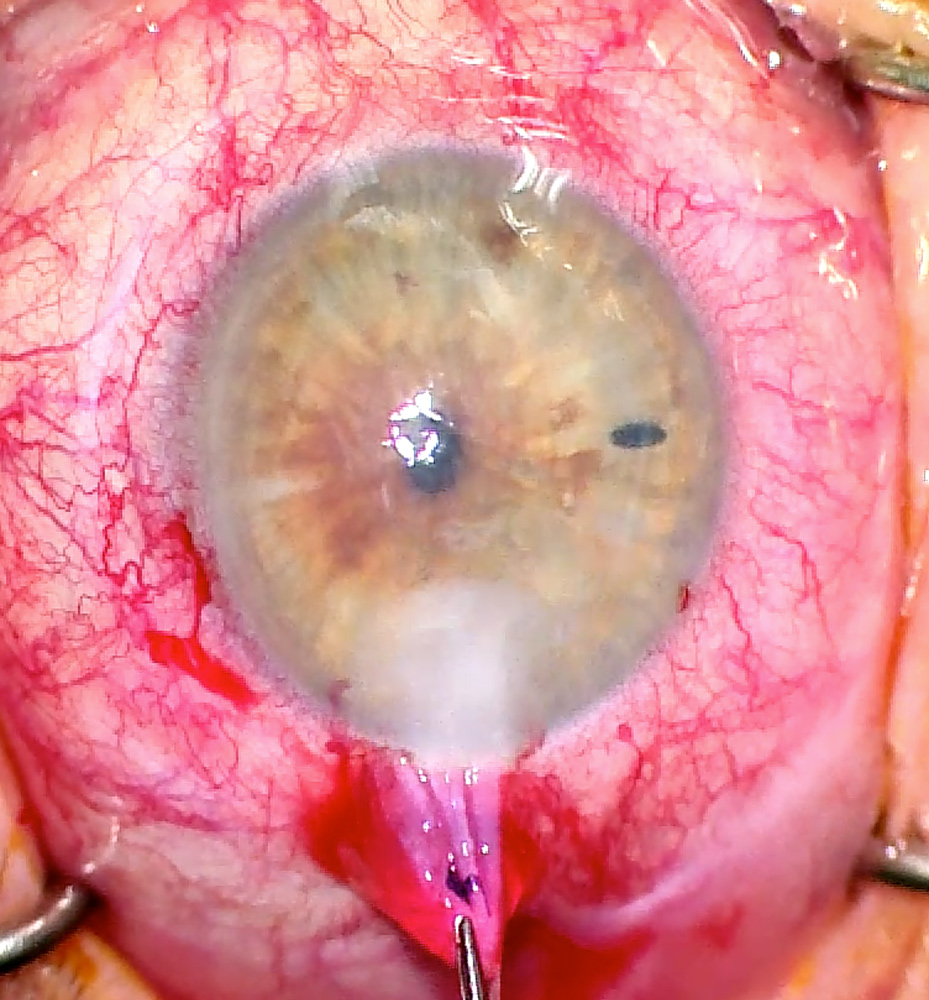
Source: Nandini Venkateswaran, MD
Source: Nandini Venkateswaran, MD
Dr. Venkateswaran said this is how she approaches her cases. “In my straightforward cases with endothelial dysfunction (i.e., Fuchs dystrophy or pseudophakic bullous keratopathy), I will perform DMEK. But since I practice in a tertiary care referral center where I’m comanaging very sick eyes with multiple ocular comorbidities and previous ocular surgeries (i.e., prior glaucoma surgeries, prior vitrectomies, iris defects, scleral fixated or anterior chamber IOL placement), I tend to perform more DSAEK as I think these complex eyes fare better with a DSAEK procedure as compared to DMEK,” Dr. Venkateswaran said.
She said she tried to learn all the different insertion techniques for DSAEK tissue, including using multiple injection devices and suturing techniques, when she was in training because she wasn’t sure what tools would be available to her when she started practice.
Source: Nandini Venkateswaran, MD
“We have excellent visual outcomes, low graft rejection rates, and less rebubbling rates with advanced DSAEK techniques,” Dr. Venkateswaran said. “I think there are some advantages to DSAEK when you’re considering your patient population, too. The higher chance of needing a rebubbling procedure with DMEK can be challenging for older patients. Gas instillation may require longer supine positioning times than air instillation, which I typically use for DSAEK cases, and compliance with positioning can be poor in patients with musculoskeletal limitations or lack of support at home. In scenarios such as these, I choose DSAEK as my go-to procedure, even if the case is relatively uncomplicated.”
It’s the shift to performing DMEK on more routine cases and DSAEK on more complex cases that Clara Chan, MD, thinks might put trainees at a disadvantage as they’re learning DSAEK.
“Cornea surgeons are performing DMEK earlier on patients with routine eyes now who have corneal decompensation since DMEK outcomes are good and the small incision surgery is lower risk,” Dr. Chan said. “DMEK tissue is also preloaded, premarked, prestripped, prepunched, so the ability to learn tissue handling and tissue preparation is limited in many programs. With the decline in DSAEK being done in routine eyes, it is now reserved for complex eyes with ACIOL, aphakia, aniridia, multiple iris defects, post-vitrectomy, etc. These cases are challenging and are often more suitable for the cornea staff surgeon to tackle. Without the opportunity to learn DSAEK in routine eyes, doing DSAEK on complex eyes is all the more challenging.”
If surgeons don’t think they have enough experience with either procedure, Dr. Venkateswaran said working with local eye banks and industry partners, attending wet labs at major medical meetings, and observing other ophthalmologists in the OR are viable options to get additional training.
Dr. Chan said even beyond DMEK and DSAEK, it’s important for cornea surgeons to know “all the procedures in the cornea surgery alphabet soup.”
“The opportunity while in fellowship to do all sorts of cases and see as much pathology as possible is invaluable,” she said. “It is much easier to learn the pearls directly from a mentor than to try to muddle through on your own once in practice when the full responsibility rests on your shoulders and there is no one there in the captain’s chair but you. In a modern cornea practice, there will still be eyes that would benefit from DSAEK, so a cornea specialist should maintain their skills in performing the procedure.”
Source: Nandini Venkateswaran, MD
Source: Nandini Venkateswaran, MD
Dr. Chamberlain said the currently enrolling DETECT multicenter, randomized, controlled trial will provide high-level evidence as to whether DMEK will outperform DSAEK in complex eyes.
“Important outcomes of this trial will be endothelial cell loss and graft survival at 6 months and 2 years,” he said. “An intriguing arm of the trial will include supplementing a randomized cohort of the patients with postoperative topical ripasudil, a rho-kinase (ROCK) inhibitor, which may promote faster corneal clearing or even longer graft survival by reducing endothelial cell stress.”
If this trial shows that DMEK outperforms DSAEK in even complex eyes, Dr. Chamberlain said we’ll see an even broader adoption of DMEK.
While DMEK is on the rise and surgeons are becoming adept at it, like the full thickness transplants and other lamellar keratoplasty techniques that came before it, someday DMEK might even become antiquated.
“Endothelial cell cultures are being developed by several entities (Aurion Biotech and Emmecell) and are now in clinical trials and may supplant some of these surgeries, if results look promising,” Dr. Chamberlain said. “Additionally, rho-kinase inhibitors and recombinant bioengineered fibroblast growth factor may be pharmaceutical agents that promote endothelial cell migration and proliferation that could be exploited to clear corneas with Fuchs dystrophy without transplanting allogeneic cells at all. These agents are in various stages of clinical trials.”
“If our technologies with endothelial cells start to gain traction, we may someday see the disappearance of all endothelial keratoplasty,” Dr. Venkateswaran said. “Many surgeons taught themselves DSAEK because the technique didn’t exist during their training; they then taught themselves DMEK. Our therapeutics are constantly advancing. Young ophthalmologists are fortunate because they currently learn DSAEK and DMEK in training. … However, what we are being trained in may grow extinct in the future.”
About the physicians
Winston Chamberlain, MD, PhD
Professor of Ophthalmology
Casey Eye Institute
Oregon Health & Science University
Portland, Oregon
Clara Chan, MD
Associate Professor of Ophthalmology
University of Toronto
Toronto, Canada
Nandini Venkateswaran, MD
Cornea and Refractive Surgery Service
Massachusetts Eye and Ear, Waltham
Waltham, Massachusetts
References
- Matsou A, et al. Microthin Descemet stripping automated endothelial keratoplasty versus Descemet membrane endothelial keratoplasty: a randomized clinical trial. Cornea. 2021;40:1117–1125.
- Rose-Nussbaumer J, et al. Descemet endothelial thickness comparison trial: two-year results from a randomized trial comparing ultrathin Descemet stripping automated endothelial keratoplasty with Descemet membrane endothelial keratoplasty. Ophthalmology. 2021;128:1238–1240.
Relevant disclosures
Chamberlain: ASLAN Pharmaceuticals, Cambium, Kowa Pharmaceuticals, LEO Pharma, Noveome Biotherapeutics, Oyster Point Pharma, Regeneron, Trefoil Therapeutics
Chan: Aurion Biotech
Venkateswaran: CorneaGen
Contact
Chamberlain: chamberw@ohsu.edu
Chan: clarachanmd@gmail.com
Venkateswaran: nandini.venkat89@gmail.com

