Glaucoma: Best practices
July 2023
by Liz Hillman
Editorial Co-Director
Optimizing ocular conditions prior to surgery is standard for any procedure, but eyes with glaucoma present some extra considerations. EyeWorld spoke with Kavitha Sivaraman, MD, and Michael Greenwood, MD, to get their insights and best practices on how to prepare eyes with glaucoma for different ocular procedures. They also shared a few intraoperative and postop considerations along the way.
In general, Dr. Greenwood said the main reason these eyes need so much attention is due to topical drop use. “These patients start taking an eye drop once a day, twice a day, then it’s multiple drops,” he said. “When they’re getting set up for surgery, their ocular surface and conjunctiva have been chronically irritated. It requires a bit of special attention for that.”
Dr. Sivaraman expounded on this, saying that preservatives in the glaucoma drops are often the culprit and noted that surgery itself and being on postop drops can further stress the ocular surface. The other issue to watch for is postoperative IOP fluctuations. She said it’s important to educate patients about the potential up front, in case glaucoma treatment might need to be escalated in response.
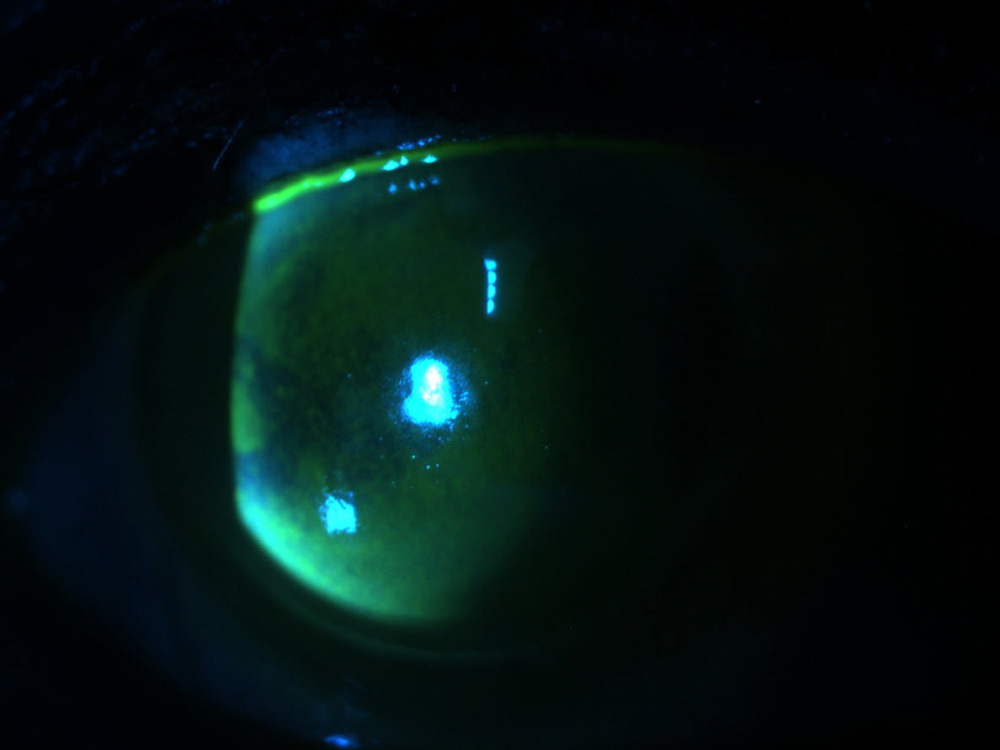
Source: Kavitha Sivaraman, MD
Glaucoma surgery
Dr. Greenwood spoke about preparing these eyes for tubes or trabeculectomy. “Because these eyes are already inflamed, you’ve got to start reversing that trend. If you’re able to get the eye to quiet down, that involves slowing down or stopping some of their glaucoma medications and starting a steroid,” he said. “You remove the agent that’s causing the inflammation and you layer on an agent that inhibits that inflammation, so you have a nice quiet eye with the hopes that they don’t over heal; if they do, it either closes off the bleb or inhibits the flow of aqueous and their pressure goes back up and the surgery has ‘failed.’”
Dr. Greenwood said reducing inflammation preop and in the early postop period is also important with the XEN Gel Stent (Allergan). For other MIGS that are not performed in conjunction with cataract surgery, he said there’s not a lot of surface prep. You do have to pay attention to where you’re doing the procedure. For example, Dr. Greenwood said the population is heavily Caucasian where he practices. For these patients who have glaucoma and are older, they often have more fat loss in the orbit, so their orbit is deeper set. Placement of the gonioprisim can be challenging.
“I use a stabilizer ring on my gonioprism to help stabilize the eye, and sometimes you need to take that off to get everything in there,” he said. “That’s one special consideration with MIGS. Trying to get a good view for MIGS can be challenging sometimes.”
Cataract surgery
For cataract surgery, Dr. Greenwood reiterated that the ocular surface of these patients is “beat up,” which can interfere with obtaining accurate measurements and thus could affect outcomes.
“If their surface is irritated, it needs to be optimized prior to doing their surgery,” he said. This could include stopping their glaucoma drops for a period of time, if they’re able to. It also can involve artificial tears, punctal plugs, and/or other dry eye treatments.
“The therapies we have for ocular surface disease are growing rapidly, and we have a lot of tools to use for each patient,” Dr. Greenwood said. “But glaucoma patients may have more inflamed lids or meibomian glands, and paying attention to that can be helpful.”
Dr. Greenwood said that if a patient cannot be taken off glaucoma medications, this is where a product like Durysta (bimatoprost intracameral implant, Allergan) could be useful. “That would be a perfect situation if you’re trying to lessen the medication burden and the patient’s glaucoma is severe enough that you can’t completely stop their medication, but you could take the topical drop off and put it inside the eye so it’s not aggravating the surface,” he said. “The postop side is another place where we’ve used it. You want to keep that inflammatory agent off the eye, and that’s where an implantable medication would work great.”
Counseling of glaucoma patients takes on other layers before cataract surgery as well. Dr. Greenwood said if they’ve had prior ocular surgery, their zonules could be weak, which requires discussion. He also said his patient population has a higher rate of pseudoexfoliation.
“Glaucoma patients in general but especially pseudoexfoliation patients are at higher risk for IOP spikes after cataract surgery, so be on the lookout for that,” he said, adding that he explains to both of these sets of patients that their healing might take longer.
Dr. Sivaraman, in addition to detailing the importance of preoperative surface prep to ensure accurate measurements, also discussed the things she prepares certain glaucoma patients for from a counseling standpoint.
“In patients with anatomically narrow angles or angle closure glaucoma, I always look at the anterior chamber depth and the density of the nucleus because the combination of a dense, thick lens with a shallow anterior chamber predisposes them to postoperative corneal edema, partly due to there being less physical distance between the ultrasound probe and the endothelium,” she said. “That becomes more significant with increasing density of the nucleus, especially if they have endothelial disease. I try to counsel patients with these risk factors that they may experience prolonged edema after surgery and potentially need a transplant later. IOL predictions also tend to be less accurate in patients with shallow anterior chambers, large lenses, and short axial length. … Although we can never guarantee glasses-free vision for any patient, it’s important for these patients to realize they may have a wider landing zone.”
Dr. Sivaraman also said the presence of a temporal peripheral iridotomy affects where she makes her incision. “I now try not to make my incision directly over the peripheral iridotomy. I find that the iris tends to be floppy in the area of the iridotomy and can prolapse more easily when the incision is made directly above it.”
Postoperative regimens can be affected by glaucoma as well. “You have to watch them closely for toxicity related to the additional preservative that you might have them on. That might be someone where you might consider using an intracameral antibiotic and skipping a postoperative antibiotic,” Dr. Sivaraman said. “You might consider doing some sort of implantable steroid. You’ve got to be careful with that though because these are the patients who are more likely to have a postoperative steroid response. Patients with a poor ocular surface, if they don’t otherwise have a lot of risk factors for CME, I might skip a prophylactic NSAID, which tends to be the biggest culprit in terms of exacerbating ocular surface disease after cataract surgery.”
Dr. Sivaraman said she likes to have optimal control of glaucoma and IOP before heading into elective cataract surgery. A high IOP could put the patient at risk for perioperative IOP fluctuations and suprachoroidal hemorrhage. “When possible, I think the best treatment is prevention,” she said.
Cornea surgery
For a surface cornea procedure, Dr. Greenwood said limiting inflammation is a factor again. “You want to be very aggressive in getting that to heal, so consider putting in permanent plugs, using a different bandage contact lens, or maybe add an amniotic membrane that will give nutrients … and get the epithelial defect to heal in a timely fashion. Maybe back off on some of the glaucoma medications so that the epithelium has the support to heal over those few days or a week,” he said.
If an endothelial transplant is needed, Dr. Greenwood said, in the setting of a tube or trab, the difficulty is getting the air bubble to stay inside the eye. “It’s a battle between how well your glaucoma device is working versus keeping the gas inside the eye,” he said. “There is a little bit more education on the front end and guiding expectations.”
He also said these eyes are at higher risk for pressure spikes, so heavy steroids might be used, but then you’re at risk for the glaucoma procedure to fail.
“There are a couple of steps, so it may not be on optimization of the eye, but education and the aftercare gets quite detailed,” he said.
Dr. Sivaraman also said that graft adherence can be more difficult in the presence of a filtering bleb or tube, and in general, the lifetime of these grafts is shorter than in an otherwise anatomically normal eye. It is important for patients to be aware that they may need repeat endothelial keratoplasty in the future.
About the physicians
Michael Greenwood, MD
Vance Thompson Vision
Fargo, North Dakota
Kavitha Sivaraman, MD
Cincinnati Eye Institute
Cincinnati, Ohio
Relevant disclosures
Greenwood: None
Sivaraman: None
Contact
Greenwood: michael.greenwood@vancethompsonvision.com
Sivaraman: ksivaraman@cvphealth.com



