ASCRS News: Eyeworld Journal Club
December 2023
by Matthew Regueiro, MD, and Chad Serels, MD
Cleveland Clinic Cole Eye Institute residents

Cleveland Clinic Cole Eye Institute Cleveland, Ohio
Healthcare inequities in the U.S. are a pervasive issue that impacts disadvantaged racial, ethnic, gender, socioeconomic, and elderly populations.1,2 Language discordance also poses a significant challenge and has a well-established relationship with sociodemographic disparities, decreased access to healthcare, and worse health outcomes.3–13 Though disparities are a well-documented challenge within the medical system, little literature exists within the field of ophthalmology. In this context, Gill et al. sought to investigate outcomes of patients with limited English proficiency (LEP) compared to those who are English proficient (EP) undergoing cataract surgery, one of the most common surgeries worldwide.
Methods
A retrospective analysis was performed using the Cataract Surgery Outcomes Database created by the Department of Ophthalmology at the University of Colorado School of Medicine. Professional research assistants trained on cataract data abstraction queried the electronic medical record to identify patients with LEP, defined as patients who self-identified as needing or preferring an interpreter during medical encounters. All patients undergoing cataract surgery between January 1, 2014, and February 24, 2020, were included in the study and were divided into EP and LEP groups.

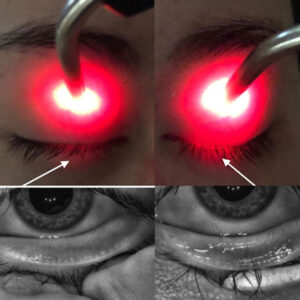
Source: Cleveland Clinic Cole Eye Institute
Demographic and preoperative characteristics were analyzed, including sex, self-reported race, ethnicity, age, preoperative corrected distance visual acuity (CDVA), uveitis, macular edema, and diabetic retinopathy. The following surgical characteristics were collected: maturity of cataract, complexity of surgery, intraoperative complications, whether a resident or attending physician was the primary surgeon, surgical time, and cumulative dissipated energy (CDE). Additionally, surgical outcomes were analyzed including postoperative complications, postoperative CDVA, change in visual acuity, refractive surprise (target refraction spherical equivalent minus postoperative refraction spherical equivalent), use of steroid eye drops at 4 weeks postop, and whether patients received subsequent Nd:YAG laser capsulotomy.
These clinical characteristics and outcomes were analyzed by LEP and EP status. Racial and ethnic subanalyses (Hispanic, African American, Asian) were performed to investigate whether associations identified within the entire cohort remained after stratification. The threshold for statistical significance was set at a P value of <0.01.
Results
A total of 13,590 eyes were included. Of these, 868 (6.4%) were identified from LEP patients. The largest two groups of LEP patients were Hispanic (39.3%) and Asian (28.2%). Compared to EP patients, patients with limited English proficiency were more likely to have a history of type 2 diabetes, macular edema, diabetic retinopathy, worse preoperative CDVA, mature cataracts, to be designated as a complex surgery, and to receive higher CDE intraoperatively. All of these characteristics were statistically significant (p<.0001). LEP patients were also more likely to have resident physicians perform their surgeries (p<.0005). Differences between LEP and EP patients with regard to complex surgeries and CDE levels remained statistically significant even after adjustment for mature cataracts (p<.0001). Postoperatively, LEP patients showed greater improvement in CDVA (p<.0001), were less likely to undergo Nd:YAG capsulotomy (p<.0001), and were more likely to be using steroid eye drops 4 weeks postoperatively (p<.0002). Subanalyses of Hispanic, African American, and Asian patients rarely revealed statistical significance due to small sample sizes; however, all of these LEP subgroups’ results trended in the same direction as the LEP cohort as a whole.
Though challenges with language discordance have been documented in other medical fields, there is limited literature within ophthalmology. The findings presented by Gill et al. exhibit preoperative, intraoperative, and postoperative disparities in cataract surgery between LEP and EP patients.
Discussion
Though challenges with language discordance have been documented in other medical fields, there is limited literature within ophthalmology. The findings presented by Gill et al. exhibit preoperative, intraoperative, and postoperative disparities in cataract surgery between LEP and EP patients.
LEP patients were more likely to have complex surgeries with a higher CDE even when adjusting for mature cataracts. Initially, this inequity may seem expected because LEP patients were more likely to have type 2 diabetes, which is associated with poor dilation and the need for iris manipulation, classifying it as a complex surgery under the authors’ definition. Interestingly, however, these associations persisted despite adjusting for type 2 diabetes and surgeon type. Additionally, Gill et al. found that LEP patients were more likely to require steroid eye drops at 4 weeks postop (p<.0002). The authors postulated this difference may be attributed to the fact that LEP patients were more likely to have complicated surgeries and higher CDE. However, the language barrier itself may have independently contributed to misunderstandings about when to taper and stop steroid eye drops.
LEP patients had a greater improvement in CDVA when compared with EP patients, without a higher complication rate. Though this largely reflects LEP patients’ more advanced cataracts due to delayed access to specialty care, it demonstrates that improving outreach can have a profound impact on these patients’ quality of life. In addition, LEP patients were less likely to undergo Nd:YAG capsulotomy, highlighting the ophthalmology community’s need for continued LEP patient education regarding posterior capsular opacification and the benefits of laser capsulotomy.
The authors noted several limitations to their study. The findings may not be generalizable as the LEP rates didn’t match the Denver metro area or the state of Colorado. Additionally, there was a large difference in sample sizes between LEP and EP groups. The relatively small LEP cohort size limited any ability for robust subgroup analysis. Furthermore, the study did not capture the modality of interpretation used, which can drastically influence a patient’s comprehension level. Finally, they did not assess other social determinants of health, such as income, insurance status, transportation, and level of education, all of which may be confounding variables.
Nonetheless, Gill et al. have illuminated the disparities that exist between LEP patients and EP patients with regard to cataract surgery. Future research is necessary to further identify and address disparities within ophthalmology.
Comparison of cataract surgery outcomes in English proficient and limited English proficiency patients
Gill ZS, et al. J Cataract Refract Surg. 2023;49:595–601.
- Purpose: To determine differences in cataract surgery outcomes between English proficient (EP) and limited English proficiency (LEP) patients.
- Setting: Sue Anschutz-Rodgers Eye Center, Aurora, Colorado.
- Design: Retrospective.
- Methods: Patients who underwent phacoemulsification at the Sue Anschutz-Rogers Eye Center between January 2014 and February 2020 were included. Patients who self-identified as needing or preferring an interpreter in medical encounters were defined as LEP. Differences in surgical characteristics and outcomes including cataract maturity, surgical complexity, and surgical complications were analyzed.
- Results: 868 eyes (6.4%) were identified from LEP patients. LEP patients were more likely to have mature cataracts (5.1% vs. 2.3%, P<.0001). LEP patients’ surgeries were more likely to be considered complex (27.8% vs. 15.3%, P<.0001) and use higher cumulative dissipated energy (mean of 9.5 [SD=9.5] vs. 7.2 [SD=7.1], P<.0001). Preoperative visual acuity was worse in LEP patients (logMAR 0.566 [SD=0.64] vs. 0.366 [SD=0.51], P<.0001) but showed greater improvement after surgery (logMAR 0.366 [SD=0.54] vs. 0.254 [SD=0.41], P<.0001). There were no significant differences in operative time, intraoperative or postoperative complications. More LEP patients were on steroids 4 weeks postoperatively when compared with EP patients (14.6% vs. 10.1%, P<.0002). LEP patients were less likely to undergo subsequent YAG capsulotomy (7.3% vs. 12.8%, P<.0001).
- Conclusions: Disparities in cataract outcomes between EP and LEP patients was demonstrated. Further research into ophthalmic health disparities for LEP patients is needed to understand the root causes and how they can be addressed.
References
- Dickman SL, et al. Inequality and the health-care system in the USA. Lancet. 2017;389:1431–1441.
- Bailey ZD, et al. Structural racism and health inequities in the USA: evidence and interventions. Lancet. 2017;389:1453–1463.
- Derose KP, Baker DW. Limited English proficiency and Latinos’ use of physician services. Med Care Res Rev. 2000;57:76–91.
- DuBard CA, Gizlice Z. Language spoken and differences in health status, access to care, and receipt of preventive services among US Hispanics. Am J Public Health. 2008;98:2021–2028.
- Fernandez A, et al. Language barriers, physician-patient language concordance, and glycemic control among insured Latinos with diabetes: the Diabetes Study of Northern California (DISTANCE). J Gen Intern Med. 2011;26:170–176.
- Fiscella K, et al. Disparities in health care by race, ethnicity, and language among the insured: findings from a national sample. Med Care. 2002;40:52–59.
- Flores G, et al. Limited English proficiency, primary language at home, and disparities in children’s health care: how language barriers are measured matters. Public Health Rep. 2005;120:418–430.
- Jacobs EA, et al. Limited English proficiency and breast and cervical cancer screening in a multiethnic population. Am J Public Health. 2005;95:1410–1416.
- Kandula NR, et al. Differences in self-reported health among Asians, Latinos, and non-Hispanic Whites: the role of language and nativity. Ann Epidemiol. 2007;17:191–198.
- Kandula NR, et al. Low rates of colorectal, cervical, and breast cancer screening in Asian Americans compared with non-Hispanic whites: cultural influences or access to care? Cancer. 2006;107:184–192.
- Timmins CL. The impact of language barriers on the health care of Latinos in the United States: a review of the literature and guidelines for practice. J Midwifery Womens Health. 2002;47:80–96.
- Wilson E, et al. Effects of limited English proficiency and physician language on health care comprehension. J Gen Intern Med. 2005;20:800–806.
- Adler NE, Rehkopf DH. U.S. disparities in health: descriptions, causes, and mechanisms. Annu Rev Public Health. 2008;29:235–252.
Contact
Goshe: GOSHEJ@ccf.org