Cataract
April 2023
by Liz Hillman
Editorial Co-Director
As advanced-technology IOLs have become more mainstream and more continue to enter the market, surgeons have refined their understanding and use of these technologies. The EyeWorld Cataract Editorial Board wanted to gain insights on the best formulas and what a reasonable adaptation period looks like with these modern IOL technologies.
EyeWorld reached out to Li Wang, MD, PhD, Linda Tsai, MD, and Kamran Riaz, MD, for their expertise in these areas.
“Formula choice is an interesting topic these days,” Dr. Riaz said. “A plethora of newer, multivariable formulas have emerged in the past few years. These formulas incorporate biometric variables besides axial length (AL) and keratometry (K), such as central corneal thickness (CCT), lens thickness (LT), and anterior chamber depth (ACD). The more recent introduction of posterior corneal power measurements, such as total keratometry (TK) with the IOLMaster 700 [Carl Zeiss Meditec], allows potentially more accurate measurements of total corneal power. Given that TK values were designed to be compatible with existing IOL formulas, significant research has gone into optimizing use of TK in regular eyes, eyes receiving presbyopia-correcting IOLs, and post-laser vision correction eyes.”

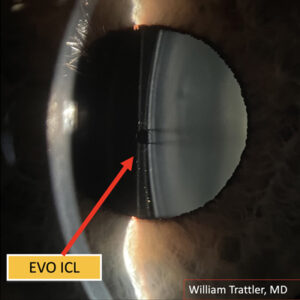
Source: Kamran Riaz, MD
While none of the physicians said that they use specific formulas for specific presbyopia-correcting IOL platforms, they had some insights to achieve the most accurate calculations.
Dr. Riaz said that total keratometry measurements in formulas may help improve outcomes with toric trifocal IOLs, but he said that the conventional keratometry is better than TK with multifocal IOLs.1,2
“I primarily use the Johnson & Johnson Vision IOL platform for presbyopia-correcting advanced-technology IOLs. For most presbyopia-correcting IOLs on this platform … I use a multivariable formula (with the ESCRS IOL Calculator) and ideally want all seven formulas to agree,” he said. “I give preference to the EVO, Barrett, and Cooke K6 formulas in case of discrepancies. I use the K values for this calculator but will use the TK values for trifocal IOLs (which I rarely do, unless the patient specifically requests them). I like to look at the Barrett TK formula that uses the TK values (on the IOLMaster 700 printout) as well for these premium IOL patients. Aiming closest to plano (even erring about 0.12 D hyperopic) is an ideal strategy since any myopic refractive error decreases objective and subjective visual function.”
Dr. Riaz said that multivariable formulas consistently outperform third-generation IOL formulas, perhaps because these formulas use biometric variables beyond just AL/K.
“I don’t think we have enough data to definitively advise that ‘formula X’ should be used with ‘IOL Y’ yet; that certainly is a topic for future research. I think that biometry technology makes a difference as well. Our group is actively exploring this idea that there are ideal combinations for formula plus IOL platform with optimized lens constants plus biometry device that remain to be identified,” he said. “It is important to stress that I do not mean to imply superiority/inferiority of a given IOL platform. However, I think the ideal triumvirate is to identify in the future that ‘formula X’ should be used with ‘IOL Y’ if you are using ‘biometry device Z.’”
Dr. Tsai said that she compares multiple formulas in order to achieve the best outcomes with advanced-technology IOLs.
“Some IOL formulas have been shown to be more accurate in certain situations like extreme axial length, post-refractive state, etc.,” she said. “I pay special attention to newer fourth-generation power calculation formulas like Barrett, Hill-RBF, and Olsen, particularly in longer and shorter axial lengths. Personalizing my IOL constants has always worked for me in the past but can be time consuming.
“If a toric platform is needed for any IOL, it is important to select a calculator that includes posterior corneal astigmatism (PCA) and surgically induced astigmatism (SIA) contributions. These are often found on the company’s website or with the Barrett Toric Calculator,” Dr. Tsai continued.
Dr. Tsai said that because she uses the IOLMaster 700, she will review third-generation formulas, but she pays special attention to fourth-generation formulas that are included with the machine’s IOL calculator, especially the Barrett formula.
“For patients who have a history of refractive surgery, I will review the Barrett True-K with TK and Haigis-L with TK, which are also included on the IOLMaster 700,” Dr. Tsai said. “Then I will compare the results with the ASCRS IOL Calculator, which has shown to be the most accurate for these patients. Occasionally, I will use the ORA System [Alcon] in patients where I think additional information is preferred to obtain the highest accuracy in my results.”
Like Dr. Riaz, Dr. Tsai said she has also recently started using the ESCRS IOL Calculator, which gives the results of the Barrett, Cooke K6, EVO, Hill-RBF, Hoffer QST, Kane, and PEARL-DGS formulas.
Once the IOL is implanted, all the physicians said there is a patient adaptation period. Dr. Wang said, “postop adaptation is a variable process that may depend both on the patient and the IOL design.” She said it usually takes between 3–6 months.
Dr. Tsai said she gives patients at least 3 months to adapt to the IOL technology, but she often encourages them to try up to a year if they’re willing. Patients might need to adapt to color changes and positive and negative dysphotopsias. She said that most patients will adapt to these visual phenomena, especially if their cataract was causing visual dissatisfaction preop.
“If they have no improvement of symptoms by 3 months and are extremely bothered by visual quality, I would start the conversation regarding a possible IOL exchange. Luckily, I have not found that I’ve had to exchange many implants due to multifocal quality complaints,” Dr. Tsai said.
Dr. Riaz said that he also asks patients to take between 3–6 months to neuroadapt.
With diffractive optics, Dr. Riaz said he considers objective measures (angle alpha being more than angle kappa) and subjective (assessment of personality types). In general, Dr. Riaz said he doesn’t recommend IOLs with diffractive optics to patients with angle alphas more than 0.4 mm. He said personality is an even larger factor in his practice.
“There are far too many practices where the surgeon only meets the patient on the day of surgery, and the IOL choice has been made by an optometrist or ancillary staff. The unhappy patients that present to clinicians are often burned by these experiences,” he said. “Assessment of patient personality (type A, engineer, high demands for near vision, etc.) and expectations are crucial and vary from patient to patient. This preop assessment is even more important than the surgery itself. The successful ‘neuroadaptation’ that happens postop begins with proper patient selection preop.”
Beyond that, Dr. Riaz said that even with proper preoperative assessment, there will be a good number of patients who need handholding, reassurance, and observation of symptoms like glare, halos, and vision that’s not meeting their expectations postop. If patients are still unhappy at 3 months and they have not had a YAG capsulotomy, he will perform an exchange for a monofocal or Eyhance IOL (Johnson & Johnson Vision).
Dr. Riaz said if the postop refraction is consistently myopic or hyperopic, residual refractive error could be to blame. Dr. Tsai said residual refractive error can contribute to complaints like night glare and blur. She said a careful manifest refraction is mandatory.
“If uncorrected refractive error is the cause, giving the patient an accurate refraction should correct the visual complaints,” Dr. Tsai said, but the bigger concerns are usually things like irregular corneal astigmatism or higher order aberrations.
Dr. Wang shared similar thoughts.
“Residual refractive error, especially residual astigmatism, may cause the postop dissatisfaction,” Dr. Wang said. “Performance of meticulous manifest refraction may determine if the postop dissatisfaction is caused by residual refraction error.”
About the physicians
Kamran Riaz, MD
Clinical Associate Professor
Dean McGee Eye Institute
Oklahoma City, Oklahoma
Linda Tsai, MD
Professor of Ophthalmology and Visual Sciences
Washington University School of Medicine in St. Louis
St. Louis, Missouri
Li Wang, MD, PhD
Professor of Ophthalmology
Baylor College of Medicine
Houston, Texas
References
- Choi A, et al. Accuracy of total corneal power calculation for multifocal toric intraocular lens implantation: swept-source OCT-based biometer vs Scheimpflug tomographer. J Refract Surg. 2021;37:686–692.
- Chung HS, et al. Comparing prediction accuracy between total keratometry and conventional keratometry in cataract surgery with refractive multifocal intraocular lens implantation. Sci Rep. 2021;11:19234.
Relevant disclosures
Riaz: None
Tsai: None
Wang: AcuFocus, Alcon, Carl Zeiss Meditec
Contact
Riaz: Kamran-Riaz@dmei.org
Tsai: tsai@wustl.edu
Wang: liw@bcm.edu