ONLINE EXCLUSIVE
Cataract
March 2022
by Liz Hillman
Editorial Co-Director
A patient presents years after cataract surgery with a dislocated IOL. Upon examination, the capsular bag is completely clear, diaphanous, floppy, and unable to support the IOL within it.
It could be dead bag syndrome.
This condition, first described by Samuel Masket, MD, is the subject of a recent paper published in the Journal of Cataract & Refractive Surgery (JCRS).1 The study’s corresponding author, Liliana Werner, MD, PhD, described the paper as the first formal peer-reviewed study on dead bag syndrome. It examined the clinical and histopathological findings of 10 suspected cases. According to the paper, eight IOLs and seven capsular bags removed due to subluxation or dislocation were included in clinical and histopathological examination.
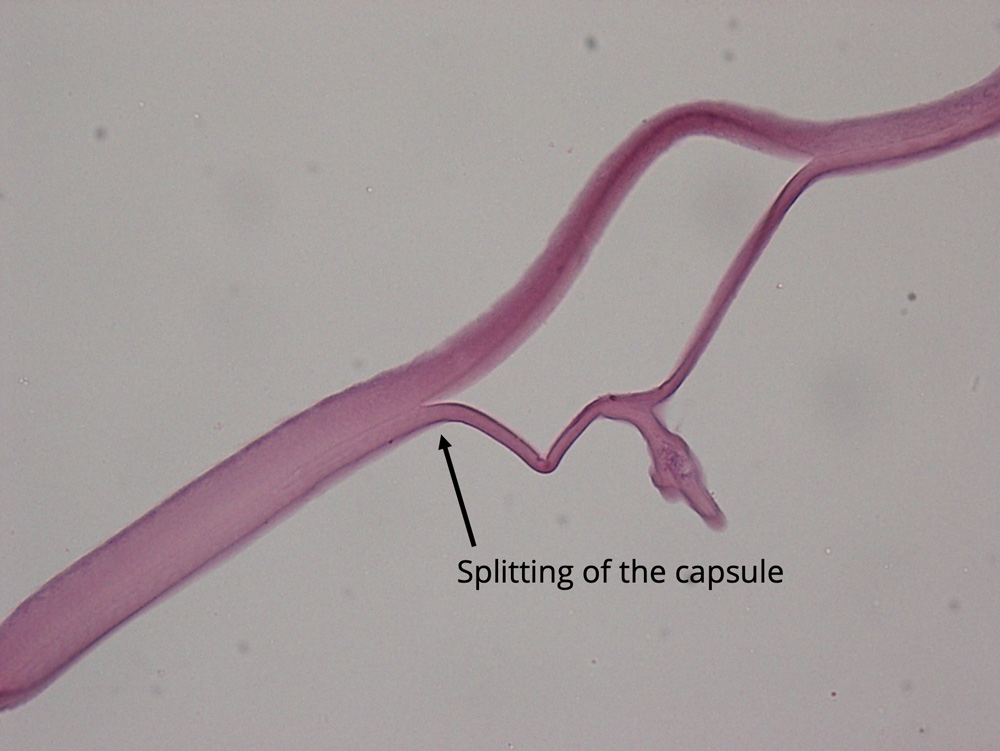
Source: Liliana Werner, MD, PhD
Culp et al. described the seven capsular bags as showing “capsular thinning and/or splitting.” The authors noted that lens epithelial cells were “completely absent on 2 specimens” and “rare” on the inner surface of the capsule of the other five. Most of the IOLs examined were unremarkable when reviewed with light microscopy, though one showed “a small amount of granular pigment deposition in the periphery.”
“In the cases included in our JCRS paper, there were no fibrotic changes or proliferative material within the capsular bag,” Dr. Werner told EyeWorld. “The main histopathological findings were capsular splitting/delamination and rare or absent lens epithelial cells attached to the capsule. It is possible that our cases represent the severe end of a spectrum, as online discussions by Steven Safran, MD, and others describe cases of possible dead bag syndrome where the capsule was floppy and delicate but still exhibited a certain amount of proliferative material within it, including abnormal gel-like Soemmering’s ring formation.”
Dr. Werner further described the possibility of varying presentations of dead bag syndrome, which were featured among the 10 suspected cases in the JCRS paper.
“There may be subluxation of the IOL inside of the floppy bag, sometimes through a peripheral defect, while the capsular bag itself is still centered. In other cases, there may be in-the-bag IOL dislocation,” she said, adding that “this syndrome does not appear to have any association with a particular IOL design or material.”
Dr. Werner also explained more about the role of the lens epithelial cells.
“Lens epithelial cells are important to the capsule as they continue to deposit extracellular matrix and lens capsule components at their basal ends, which contributes to the thickening of the capsule throughout life, as well as maintaining its integrity,” she said. “On the other hand, the capsule is also important to the lens epithelial cells. It represents an anchor point for the basal surfaces of the cells, also providing necessary signals for proper lens cell proliferation, migration, and differentiation. Therefore, in dead bag syndrome there may be a problem in the cells, which degenerate affecting the capsule, or a problem in the capsule itself, initiating a cycle of damage to the cells with further damage to the capsule. The exact etiology is still unknown, and further formal studies are necessary to better understand this condition.”
In terms of prevalence, Dr. Werner said the condition is not that common. Discussions with those who are aware of the syndrome, she noted, say they see at most five cases per year. But practices that frequently manage dislocated IOLs might see a higher rate, about one a month or even more.
In general, Dr. Werner said the rate of postop in-the-bag IOL dislocation is reportedly increasing. Predisposing conditions for this are pseudoexfoliation and other conditions associated with progressive zonular weakening. As of right now, however, there are no known risk factors for dead bag syndrome.
“In dead bag syndrome, signs of zonular weakness are usually absent in the original IOL implantation procedure, based on the cases described in the JCRS paper, and we hypothesize that late postoperative zonular failure is related to capsule splitting/delamination occurring at the level of zonular attachments,” Dr. Werner said.
Dr. Werner said the JCRS paper has already helped raise awareness about dead bag syndrome, with many surgeons reaching out to say they’ve had cases that were likely dead bag syndrome. Prior to the paper, there have been videos presented at society meetings and informal discussions on listservs on the topic.
“When looking at the results of our study, especially regarding the scarcity of lens epithelial cells in the capsules, surgeons are naturally asking the question about a possible relationship with capsular polishing,” Dr. Werner said. “There has been a lot of emphasis on polishing techniques to prevent capsular bag opacification/fibrosis, especially in association with premium lenses. However, even extensive polishing cannot completely remove all lens epithelial cells, and polishing is usually not done at the capsular bag equator, as this region is not readily visible. Therefore, to date there is no established association between capsular polishing and this condition.
“There are many unanswered questions not only about the etiology of this syndrome but also in its manifestations. It is therefore fitting that management is advised on a case-by-case basis, depending on presentation, as well as status of the zonular support,” Dr. Werner said.
About the physician
Liliana Werner, MD, PhD
Professor of Ophthalmology and Visual Sciences
John A. Moran Eye Center, University of Utah
Salt Lake City, Utah
Reference
- Culp C, et al. Clinical and histopathological findings in the dead bag syndrome. J Cataract Refract Surg. 2022;48:177–184.
Relevant disclosures
Werner: None
Contact
Werner: Liliana.Werner@hsc.utah.edu



