Cataract
April 2022
by Liz Hillman
Editorial Co-Director
A patient comes in for a postop visit unhappy with their vision after they’ve received a presbyopia-correcting IOL—now what?
Tal Raviv, MD, said that his practice is doing more presbyopia-correcting IOL surgeries than ever before with the latest generation of lenses. While many patients are pleased with their outcomes postop, not every patient is thrilled. “We needed a way for all of our doctors to be able to compassionately and effectively treat any patient who needed extra care,” Dr. Raviv said.
So he created an algorithm—the Raviv “Getting to Happy” Post-IOL Algorithm—to help guide physicians through the process of managing a patient who is unhappy with their presbyopia-correcting IOL.
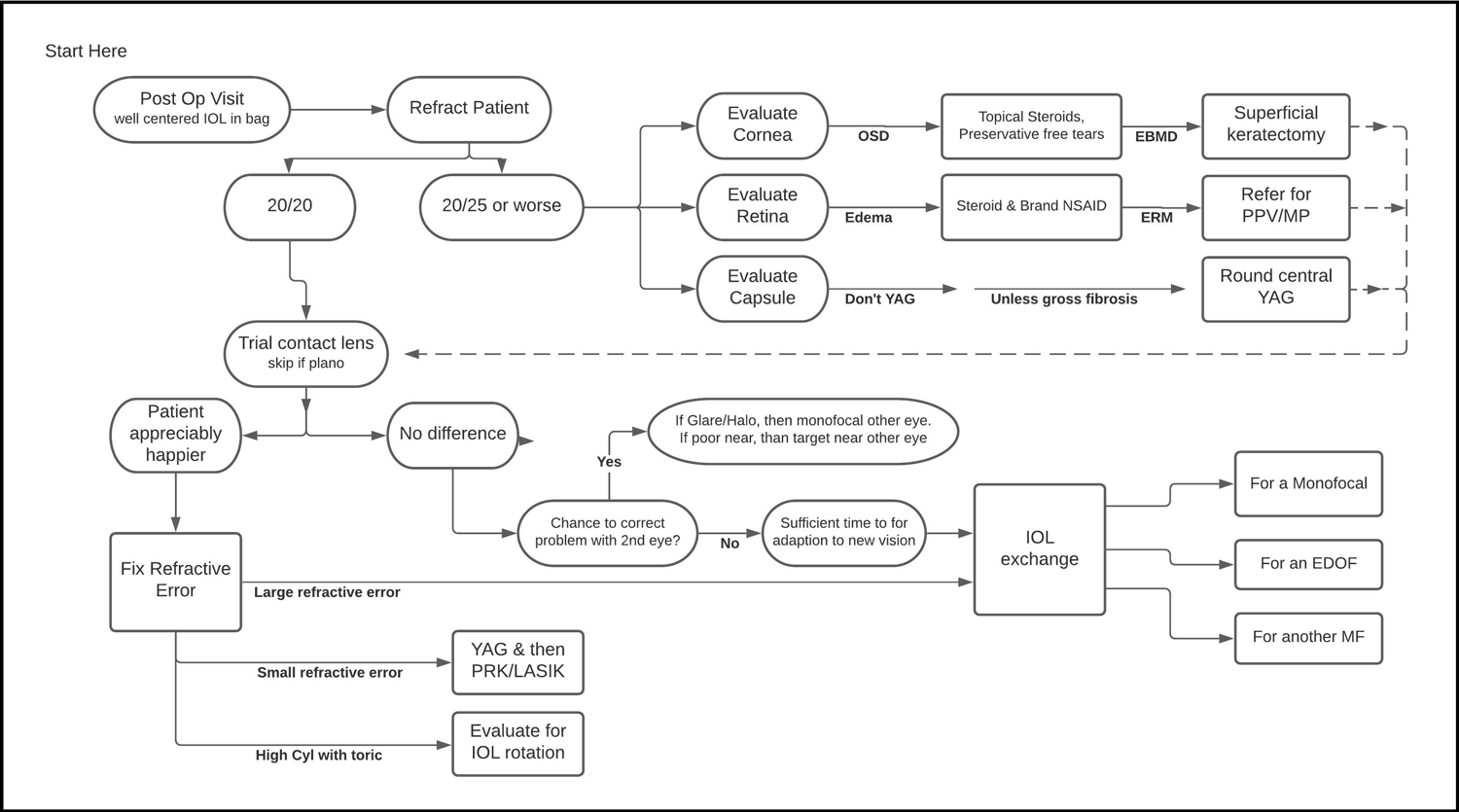
Source: Tal Raviv, MD
“I would estimate about 10% of premium IOL patients have some issue, with about three quarters of those able to be resolved medically or by choosing another IOL in the fellow eye and the rest needing some form of enhancement, such as PRK/LASIK or IOL exchange,” Dr. Raviv said. He added that he tells presbyopia-correcting IOL patients that about 3–4% will need an enhancement. “I see a number of unhappy post-refractive patients who are coming in for a second opinion following surgery elsewhere.”
Dr. Raviv’s algorithm starts at the postop visit with a well-centered IOL in the bag. From there, refract the patient and follow the paths based on the outcome of the refraction and subsequent testing.
In general, Dr. Raviv said it’s critical to teach patients interested in presbyopia-correcting IOLs preop that “even with the most exacting surgery and latest generation of customized IOLs, there is a small likelihood of needing an enhancement procedure.”
“There are some patients who tell us preoperatively that they don’t ever want a second surgery, and in those we rule out a multifocal IOL,” Dr. Raviv continued. “Our profession still can’t get to 100% within ±0.25 D with any presbyopic IOL solution, so enhancements are critical.”
Case example
Dr. Raviv provided a case to illustrate how he used his algorithm. Three weeks after receiving a trifocal toric IOL, a patient was in his office complaining of a “film” and “blurry/hazy” vision. Dr. Raviv said the patient had some dry eye preop and had been on topical cyclosporine for a month. First, he refracted the patient. She was correcting to 20/25- with a slight myopic correction.
“Since the BCVA wasn’t a crisp 20/20, we pursued treatment to improve the vision,” he said, noting that OCT showed the macula was flat and unchanged and there was no significant PCO. “There was some punctate corneal staining. The topical steroid was increased and NSAID was discontinued. Restasis [cyclosporine, Allergan] and preservative-free tears were maintained.”
At 2 months postop, the patient’s BCVA with a –0.75 D improved to 20/20. From there, Dr. Raviv did an in-office contact lens trial, in which the patient noted significant improvement in distance and near vision. The plan was to continue dry eye drops for a few months, then proceed with PRK.
At postop month 4, BCVA was 20/40- and 1+ PCO was present. A YAG capsulotomy was performed followed by another refraction. Dr. Raviv then performed PRK. One month after PRK, the eye was plano 20/20 (and J2), and the patient was very happy, Dr. Raviv said.
Other perspectives
Blake Williamson, MD, shared his perspective on patients who are unhappy after cataract surgery. He said the question is in what percent of the lenses that you place is there unhappiness such that the surgeon needs to do something about it? Dr. Williamson said his explant rate is less than 1%.
“I think that’s a testament to how we educate the patients on the preop side, making sure they understand the limitations, set appropriate expectations, pick the right patients, etc.,” he said, adding that if surgeons are using presbyopia-correcting lenses, they should have the skills to explant or perform a touch-up or be prepared to refer should the need arise.
Reasons for patient unhappiness can be any number of things. Dr. Williamson said often it’s an issue between eyes.
“It’s like having a cowboy boot on one foot and a roller skate on the other. … Everything is off because they need to have the other eye done,” he said. “We educate them on the front end and let them know they’re not going to love [the time] between eyes.”
Other issues include glare and halo in the early postop period. Dr. Williamson said patients need to be reminded that it can take 3–4 months for them to neuroadapt. Another issue could be that the patient doesn’t love their near vision. They might like it but not love it, Dr. Williamson said. The same issue could happen with distance. It might be a case where mixing and matching IOLs could help.
Dr. Williamson said he doesn’t think of these as complaints from patients but rather observations. He said he listens to these observations and often uses them to inform what the best course of action is for the second eye.
Douglas Koch, MD, discussed the challenge of cataract surgery in patients who have had prior refractive surgery. These patients elected for spectacle independence with initial refractive surgery, so they might have the same expectation after cataract surgery, if they’re opting for a presbyopia-correcting IOL. Dr. Koch said that these patients often have multifocal corneas whose depth of focus can compensate in part for residual refractive error, but it’s not uncommon for them to be off target, and residual refractive error is more problematic with most EDOF and multifocal IOLs. It’s especially important that these patients be educated about the added challenge their prior refractive surgery poses for hitting the post-cataract surgery refractive target, Dr. Koch said. He thinks that the Tecnis Symfony lens (Johnson & Johnson Vision), with its large “landing zone,” is more forgiving in this regard, and in his practice he largely avoids other EDOF and multifocal IOLs in post-refractive eyes.
If the needed postop correction is small, Dr. Koch said he’ll propose PRK. Usually LASIK is not feasible, but sometimes he will do a flap recut and lift, if the cornea is amendable to further flap surgery. For residual refractive error of –2 or more or +1.5 or more, he prefers IOL exchange.
As for taking lessons learned from the first eye and applying them to the second, Dr. Koch said it’s more nuanced in post-refractive surgery patients. “If they’ve had a modest LASIK, you could probably learn something from the first eye, but if they’ve had a large LASIK correction, and especially in post-RK eyes, one cannot rely as much on the outcome of the first eye when calculating the IOL for the second one,” he said.
Dr. Williamson said that patients who are unhappy with their refractive outcome want to be heard and confident that their surgeon is understanding and has a plan for them. He said the staff often has an accurate pulse on just how unhappy a patient might be (e.g., the patient might be more honest with the staff than the physician). Dr. Williamson said it’s important to remind the patient with a presbyopia-correcting IOL of what they do have—“awesome near vision”—and at 3 months postop consider more significant action if they’re still not happy, such as a YAG capsulotomy (don’t YAG too early, Dr. Williamson cautioned) or explant.
“Never do [an explant] before a month unless it was a refractive miss,” he said. “If you hit the refractive target … but the patient is unhappy with side effects, give it at least a month, then get it out and refund.”
About the physicians
Douglas Koch, MD
Department of Ophthalmology
Cullen Eye Institute
Baylor College of Medicine
Houston, Texas
Tal Raviv, MD
Eye Center of New York
New York, New York
Blake Williamson, MD
Williamson Eye
Baton Rouge, Louisiana
Relevant disclosures
Koch: Alcon, Carl Zeiss Meditec, Johnson & Johnson Vision
Raviv: Johnson & Johnson Vision
WIlliamson: Johnson & Johnson Vision
Contact
Koch: dkoch@bcm.edu
Raviv: talraviv@eyecenterofny.com
Williamson: blakewilliamson@weceye.com



