Cornea
December 2021
by Liz Hillman
Editorial Co-Director
Less than 10 years ago, the idea that you could preserve vision and achieve corneal clearance in a patient with Fuchs without donor tissue was met with skepticism. Now, this idea is increasingly accepted, adopted, and is being more widely researched with a clinical trial underway for a pharmaceutical to aid in cell migration.
Descemet’s stripping only (DSO), where a descemetorhexis is made in Descemet’s membrane without keratoplasty, was introduced in the mid-2010s. Kathryn Colby, MD, PhD, said when she started talking about it in 2016, she “wouldn’t go so far as to say … that people threw tomatoes at me, but almost.”
“Around 5 years ago the high variability in patient outcomes was a barrier to widespread adoption of the technique,” said Greg Moloney, MD, also an early proponent and researcher of DSO. “Patients and surgeons were often unwilling to embark on a surgical journey that had an unknown timeline and might eventually result in a graft in any case.”
What’s changed?
In more recent years, there have been published reports of improvements in clearance rates and time to clearance, Dr. Moloney said, noting that it likely relates to several factors.
“It seems clear now that patient selection should be limited to those with central corneal disease. The need for a healthy peripheral cell reservoir is understood based on long-term studies of outcomes that illustrate cell migration as the primary driver of clearance,” he said.
What’s more, surgical technique has improved with the understanding that stromal trauma can be counterproductive to cell migration, and preliminary data support the role rho-kinase (ROCK) inhibitors can play in cell migration.
“Despite all these advancements, there are patients who will fail to clear despite good selection, good surgery, and the use of supplemental ROCK inhibitors,” he said, adding, “Those considering a DSO should be prepared to accept a DMEK as an eventual consequence.”
In terms of outcomes, Dr. Moloney said he has cared for patients with multiple endothelial grafts in the fellow eye who were treated with DSO in the ungrafted eye, with equivalent visual results.
Dr. Colby offered a similar perspective as Dr. Moloney when it comes to patient selection and surgical technique. Patients, she said, should have primarily central Fuchs, with guttae in the center (no more than 5–6 mm, though 4–5 mm is better) and preserved peripheral endothelium. She said the peripheral endothelium can be evaluated with a confocal microscope or a specular microscope that can go to the paracentral area or by clinical exam using 40x magnification on the slit lamp.
“Someone who has limbus to limbus guttae is not a candidate for this. And they have to be symptomatic,” she said. “People come to me wanting to have this prophylactically. They have to have symptoms because if it doesn’t work, you need to do a corneal transplant.”
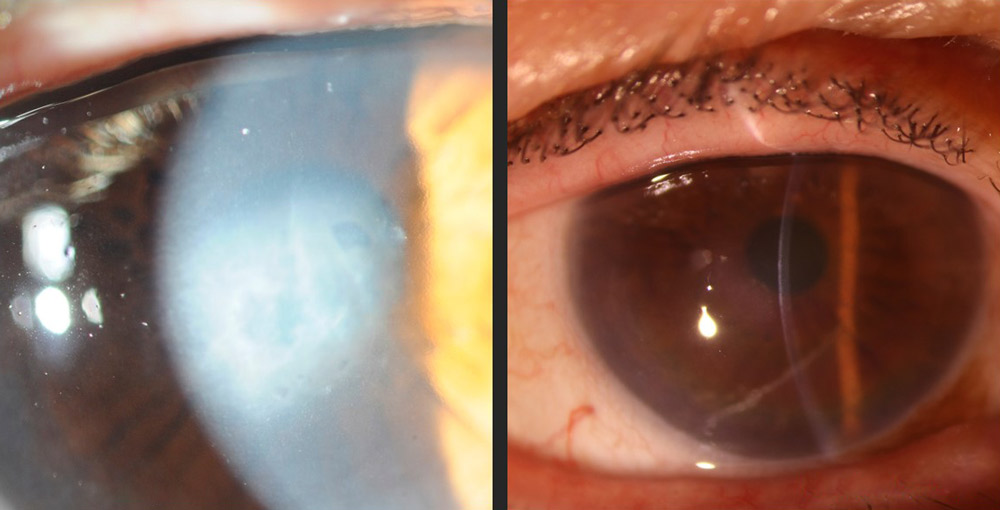
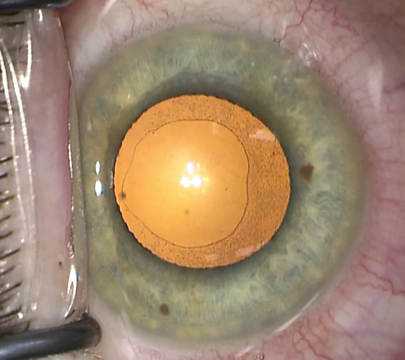
Source (all): Gregory Moloney, MD
Dr. Colby said the patient needs to be able to endure the 2–3 weeks of corneal edema postop, and as such, she usually doesn’t do DSO on monocular patients.
Surgically, she said we know now that a smooth-edged tear is better than a jagged-edged tear. Dr. Colby said she uses blunt-tipped Gorovoy forceps (Moria).
“They’re good for making the break into Descemet’s membrane atraumatically, and it’s easy to pull the Descemet’s membrane and endothelium around and do a descemetorhexis,” she said.
She also said surgeons need to be careful to not dig the instrument into the posterior stroma because it will cause scarring. Though not often visually significant, Dr. Colby said surgeons don’t like to see scarring.
Overall, Dr. Moloney said there is a greater understanding, due to knowledge gained from the surgical journey of DSO, for the mechanisms and limitations for corneal clearance after endothelial trauma. This, he said, will serve the community well as we embark on the next surgical phase of cell replacement therapy.
ROCK inhibitors
Though reports have shown enhanced endothelial cell migration with the use of a ROCK inhibitor, there is not one approved for this indication in the U.S. Netarsudil (Rhopressa, Aerie Pharmaceuticals) is approved for reducing IOP but has been found in some cases to help in corneal clearance. Use of netarsudil after DSO for endothelial cell migration would be off label, Dr. Colby said.
However, a Phase 2 trial evaluating a different ROCK inhibitor, ripasudil, for DSO is underway. The compound is already approved for use outside of the U.S. for glaucoma as Glanatec (Kowa). The study sponsored by the Kowa Research Institute has completed patient enrollment and is expected to have topline data in December 2021. Between 60–65 patients were enrolled in this double-masked, randomized, placebo-controlled 12-week trial that evaluated safety and efficacy of ripasudil (known as K-321 in the study) after DSO in patients with Fuchs, Dr. Colby said. The investigational drops were administered BID or QID with the central endothelial cell density being the primary outcome measure and number of participants with at least one adverse event the secondary outcome measure.
Dr. Colby, the U.S. chair of the Kowa study, said if the results from the Phase 2 trial are positive, a Phase 3, FDA-approval trial could begin in 2022. Unable to speak to the Kowa trial data, Dr. Moloney, who consulted on the design of the trial, said anecdotal evidence and other small to medium trials have supported the role of ROCK inhibitors in promoting cell migration after DSO.
“The observation of ‘relapse edema’ on cessation of the drop in some patients post-DSO is strong clinical evidence of the drug effect,” he said. “In vitro and in vivo results also suggest that not all patients require ROCK inhibitors to achieve corneal clearance. Determining who best benefits from ROCK inhibitors and especially at what dose requires a well-constructed, controlled, prospective clinical trial. The Kowa study is meeting this need.”
In general, Dr. Moloney said having an alternative procedure to treat a subset of patients with Fuchs without a transplant has been “extremely gratifying.” While he said the technique hasn’t replaced DMEK for all Fuchs patients, in the way DMEK replaced DSEK, “for appropriately selected patients, I think it provides a better surgical journey.”
About the physicians
Kathryn Colby, MD, PhD
Elisabeth J. Cohen Professor and Chair
Department of Ophthalmology
New York University Grossman School of Medicine
New York, New York
Greg Moloney, MD
Clinical Associate Professor
University of British Columbia
Vancouver, British Columbia
Relevant disclosures
Colby: Kowa has a research contract with New York University for Dr. Colby’s services as U.S. chair for the K-321 clinical trial
Moloney: Kowa
Contact
Colby: Kathryn.Colby@nyulangone.org
Moloney: gregorymoloney@yahoo.com.au



