Cornea
July 2021
by Liz Hillman
Editorial Co-Director
Underdiagnosed, often neglected, and much more common than clinicians realize is how some physicians describe conjunctivochalasis.
Patients with symptomatic conjunctivochalasis often complain of dry eye and receive treatment that doesn’t resolve their symptoms. Often the system ends up pushing these patients to cornea specialists who ultimately discover the condition, make the diagnosis, and determine a course of treatment.
“We [need to] start by understanding that this is a significant clinical entity. It’s not rare, and it should be in your differential diagnosis of ocular surface disease,” said Edward Holland, MD.
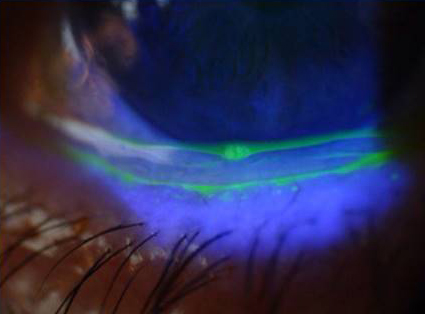

Source: Edward Holland, MD
Tanya Trinh, MBBS, FRANZCO, said a review of conjunctivochalasis concluded that the condition most commonly affects elderly patients, although it can be seen in a wide range of ages. She said its precise prevalence in the U.S. is not known, but some reports have shown higher prevalence in Asian populations.
“Not all cases of conjunctivochalasis are clinically significant, and non-standardized diagnostic criteria likely contributes to the wide variance in reported prevalence rates,” Dr. Trinh said. “It is also likely underdiagnosed because patients typically will come in presenting with dry eye symptoms and ocular irritation and it is only upon examination and work-up that it is discovered; patients typically are not referred straight in with this diagnosis.
Underdiagnosis also occurs because a large proportion of patients with this condition are asymptomatic,” Dr. Trinh continued. “If patients are experiencing symptoms, they most often complain of dryness, discomfort, blurred vision, fatigue, pain and burning, foreign body sensation, and episodes of tearing,” she said.
According to Nambi Nallasamy, MD, who wrote about conjunctivochalasis on the website of the American Academy of Ophthalmology, “no true etiology has been determined” for the condition.1 He noted several studies that suggest mechanical causes, observe the overexpression of inflammatory metalloproteinases and inflammatory cytokines, and describe how conjunctivochalasis affects tear meniscus formation and blocks tear movement from the fornix.2–5
Diagnosing conjunctivochalasis
Dr. Holland called conjunctivochalasis a diagnosis of exclusion.
“On the initial visit, I do not recommend the definitive treatment for conjunctivochalasis, which is surgery for most significant cases. What I recommend is to rule out the more common causes of ocular surface symptoms: Does this patient have aqueous tear deficiency? Does this patient have MGD? Any findings of allergic conjunctivitis? I will treat those conditions if they’re present because patients can have conjunctivochalasis and not have symptoms related to it. If the standard treatment of the common causes of ocular surface disease fail, then I know I have ruled out the more common diagnoses and I can be more certain that conjunctivochalasis is the cause of the patient’s symptoms and we can discuss possible surgery,” he said.
Dr. Trinh said point-of-care testing might have a role in evaluating conjunctivochalasis in looking for associated ocular surface inflammation. “[T]he diagnosis of [conjunctivochalasis] is reliant on a careful slit lamp examination and especially observation of the patient during the blinking phase,” she said.
John Hovanesian, MD, said a clue that a patient could have conjunctivochalasis and not just dry eye is localized pain.
“Often patients can point with one finger where it hurts. … Of course, that can be a number of different things, but when you see that, you have to pay attention. They’ll often report it when they blink,” he said.
Dr. Hovanesian described his “thumb test” where he’ll put his thumb on the patient’s lower eyelid below the lashes in the area where they’re reporting pain and ask them to look around. If they say that’s producing pain, it’s a clue into conjunctivochalasis.
Clifford Salinger, MD, said that fluorescein stain and a yellow filter are his most helpful tools in visualizing the rugae and redundant conjunctival folds, and punctate conjunctival staining, which he thinks are the causes of many of the symptoms associated with this condition. Dr. Salinger described conjunctivochalasis as a form of “mechanical dry eye” where the normal position of the inferior tear meniscus is blocked by the redundant conjunctival folds, and the tear reservoir in the inferior cul-de-sac is also compromised by the presence of loose Tenon’s fascia and redundant conjunctiva. Without an area for the tear meniscus and tear reservoir to reside, there is not enough reserve tears and lubricants for the eyelid to pull up over and across the eye with each complete blink, thus contributing to the dry eye condition.
Medical management
Dr. Holland said unless the conjunctivochalasis is severe and very symptomatic, he recommends treating other common ocular surface disease issues first because almost all of his patients with conjunctivochalasis have some degree of MGD.
“What I find is when I manage their MGD, a lot of their symptoms go away, and we don’t surgically manage their conjunctivochalasis in many cases. On the other hand, a lot of patients have been on dry eye therapy for years and they’re not happy, and when I finally surgically manage their conjunctivochalasis, their symptoms vastly improve,” he said.
Dr. Hovanesian said his first line of defense is lubrication, followed by optimizing any dry eye conditions that can coexist with conjunctivochalasis. He said he’s had limited success with nonsteroidals, Prolensa (bromfenac, Bausch + Lomb) in particular.
Dr. Salinger explains to each patient the diagnosis at the outset, using pictures of their own eye to help the patient visualize the problem. While surgical options are not primary treatment, he at least informs the patient of the potential for future surgery to mitigate symptoms. His first step in treating conjunctivochalasis is educating the patient, teaching them about environmental triggers to avoid, addressing inflammation and any meibomian gland dysfunction/blepharitis. For inflammation, Dr. Salinger said he prefers loteprednol products, and for MGD he recommends hot compresses, lid massage, gentle lid cleaning, adding Avenova (hypochlorous acid, NovaBay Pharmaceuticals) when indicated, HydroEye (ScienceBased Health), an omega-3/omega-6 supplement, azithromycin or doxycycline either topically or systemically, and/or LipiFlow (Johnson & Johnson Vision).
If symptoms are not improved with these treatments by the second visit, Dr. Salinger addresses aqueous production, performing a Schirmer’s test and considering punctal occlusion or immunomodulator medications like Cequa (cyclosporine, Sun Ophthalmics), Xiidra (lifitegrast, Novartis), or Restasis (cyclosporine, Allergan). After 3–4 visits, and possibly 4–6 months of treatment, if significant symptoms still persist, that’s when Dr. Salinger revisits a formal discussion about surgical options.
Surgical management
Dr. Holland resects the inferior conjunctiva 180 degrees or, if needed, will do a full 360-degree resection. He won’t do a 360 resection if the patient has glaucoma and might need glaucoma surgery in the future.
Dr. Holland said he takes out the strip of loose conjunctiva, taking care to avoid the limbus. He’ll often do the patient’s second eye as well because it’s frequently a bilateral condition. He said that he doesn’t use amniotic membrane but knows other surgeons advocate for it.
“My surgical technique is to not resect too much conjunctiva that you have a defect you need to fill in because I’d rather leave conjunctiva than put in amniotic membrane. Only resect the amount of conjunctiva you need and advance the remaining conjunctiva to close the defect,” he said.
Dr. Trinh said her preferred technique is “the paste-pinch-cut conjunctivoplasty,” which she noted was reported by Linden Doss, MD, and colleagues in 2012.6
“It involves the use of a fibrin sealant that is injected under the conjunctiva in a linear fashion below the limbus,” she explained. “The conjunctiva is then ‘pinched’ together with a pair of curved tying forceps where the excess conjunctiva is gathered into a ridge while the sealant polymerizes. The now everted ridge of excess conjunctiva and sealant is resected with Westcott scissors.
“We prefer this technique because it allows a pleasing cosmetic outcome as well as reduced bleeding. Care should be taken to adequately assess the amount of excess conjunctiva that is to be resected to avoid forniceal shortening.”
Dr. Hovanesian described other methods. One can be done in the office with topical anesthetic. He said using low-temperature cautery to burn a grid pattern in the conjunctiva a few millimeters apart in the area of looseness creates scarring that tethers the conjunctiva to the underlying globe. For patients with a limited amount of conjunctivochalasis, this can be effective, he said. For more extensive conjunctivochalasis, Dr. Hovanesian described his technique, which includes covering the area of excised conjunctiva with dehydrated amniotic membrane (Ambio2, Katena).
Dr. Salinger prefers to use a cryopreserved amniotic membrane product (Bio-Tissue) for his surgical management of conjunctivochalasis. He said when he performed surgery without the cryopreserved amniotic membrane, the areas of resection were slow to heal and there were large areas of bare sclera that could develop dellen or scleral melting.
His pearls for surgical management include: 1) Start 2–3 mm peripheral to the corneal limbus, avoiding the limbal stem cells, and making a semicircular incision, dissect deep into the inferior cul-de-sac. 2) Remove as much loose Tenon’s fascia as possible with the goal of reforming the inferior cul-de-sac, paying special attention to the area of the inferior puncta that might have been blocked by loose, redundant conjunctival folds draped over the punctal opening. 3) After resection, cauterize with bipolar cautery to seal the gap, similar to excision of pterygium with amniotic membrane and ocular reconstruction. Dr. Salinger credited Neel Desai, MD, with the importance of cautery in this step, as it prevents prolapsed orbital fat from getting in the way when it’s time to place the amniotic membrane. 4) Cut the amniotic membrane into a smaller and a larger piece. Dr. Salinger glues the smaller piece in position over the inferior rectus muscle, then places the larger piece of the amniotic membrane covering the entire area of resection and inferiorly deep into the inferior cul-de-sac, gluing the larger piece in position, first the nasal half, then the temporal half. He gently pulls the edge of the resected conjunctiva forward over the amniotic membrane, and places a few absorbable sutures around the periphery and inferiorly through both the conjunctiva and the amniotic membrane to anchor everything in place and inferiorly to reform the inferior cul-de-sac.
“What we’re left with is a broad horizontal band of exposed amniotic membrane measuring approximately 6–8 mm vertically,” Dr. Salinger said.
A change in understanding
Dr. Desai said just the term conjunctivochalasis creates some misunderstandings as to what it is and how he thinks it should be treated. The first part of the name suggests an issue with the conjunctiva and the second half suggests excess. Dr. Desai said conjunctivochalasis is a misnomer for the condition, which at its root is an issue with the underlying Tenon’s fascia becoming dissolved and atrophic due to chronic inflammation, such as factors like MMP-9 and other inflammatory mediators common in patients with chronic dry eye. As Tenon’s becomes dissolved, the conjunctiva becomes loose and slides around, he explained. The normal tissue barriers that would prevent orbital fat prolapse are dissolved as well. This fat can prolapse into the fornix causing it to become foreshortened and filled by loose conjunctiva and orbital fat.
“Chalasis” suggests an excess of conjunctiva when there’s not, in fact, “extra,” it’s just loose, Dr. Desai said. For this reason (and several others), Dr. Desai uses amniotic membrane in his surgical management for conjunctivochalasis. If one were to remove a strip of conjunctiva and not replace it with amniotic membrane or another platform, he said there might be short-term improvement, as loose conjunctiva would no longer create a foreign body sensation. Over the long term, however, Dr. Desai said it doesn’t improve adherence of the conjunctiva, doesn’t address prolapsed orbital fat, doesn’t improve the inflammatory condition of the eye and goblet cell deficiency, and can exacerbate a conjunctival deficiency.
Dr. Desai said that amniotic membrane allows for reconstruction of the cul-de-sac, creates a barrier against prolapsed orbital fat, addresses Tenon’s insufficiency, and allows for regenerative healing with the biologics inherent in the membrane.
Continued need for education
Dr. Hovanesian said there’s still a need for simple awareness about conjunctivochalasis.
“Every eyecare provider is seeing conjunctivochalasis and needs to be aware of it so you can optimally treat these patients because otherwise, they tend to go from doctor to doctor unhappy with their treatment and having their problem unsolved,” he said.
Dr. Desai said awareness about the condition in general is still needed, as is a better understanding of what the condition is and the right approach to its management.
“We are facing an uphill battle in terms of making more surgeons aware of even looking for it, understanding what the condition is, and having the right approach to it. All three of those need a lot of work,” Dr. Desai said.
ARTICLE SIDEBAR
More from Dr. Hovanesian
Dr. Hovanesian described conjunctivochalasis, its diagnosis, and management in a video (bit.ly/2SGz4Ho).
Surgically, after the physician has identified where the areas of loose conjunctiva are, Dr. Hovanesian showed how to excise a small strip of conjunctiva 1 mm from the limbus so as to not disturb limbal stem cells. He then cuts dehydrated amniotic membrane to the same shape of the conjunctival defect, making it 1–2 mm larger on all sides except the corneal side.
“We use dehydrated amniotic membrane because of the ease of cutting with the packaging and the ease of application directly on to the eye in its dry state,” he said.
From there, fibrin adhesive is applied in two layers. After applying the second adhesive, the graft is applied and placed under the surrounding conjunctiva.
Postop, Dr. Hovanesian prescribes prednisolone acetate 1% QID, fluoroquinolone antibiotic QID, and a topical nonsteroidal.
In before and after pictures, Dr. Hovanesian noted less inflammation and complete coverage of surface epithelium after healing.
He also said a review of his patients over the course of a year identified eight patients with conjunctivochalasis. All patients were older than 5 years, had a history of prior eye surgery, and previous diagnosis of severe dry eye. Dr. Hovanesian said all of these patients had excision of the affected conjunctiva and placement of the dehydrated amniotic membrane, which resulted in complete resolution of the symptoms following surgery.
“We encourage our colleagues to consider conjunctivochalasis in patients who have been previously diagnosed with unremitting dry eye that is associated with pain. Naturally, making every effort with nonsurgical therapy is an appropriate first step in this condition, but when conservative treatment fails, we have had very good success using the described technique,” Dr. Hovanesian said in the video.
About the physicians
Neel Desai, MD
The Eye Institute of West Florida
Tampa, Florida
Edward Holland, MD
Professor of Ophthalmology
University of Cincinnati
Cincinnati, Ohio
John Hovanesian, MD
Jules Stein Institute
University of California, Los Angeles
Los Angeles, California
Clifford Salinger, MD
VIP Laser Eye Center
Palm Beach Gardens, Florida
Tanya Trinh, MBBS, FRANZCO
Mosman Eye Centre
Sydney Eye Hospital
Sydney, Australia
References
- Nallasamy N. Conjunctivochalasis. American Academy of Ophthalmology. eyewiki.aao.org/Conjunctivochalasis. Accessed Nov. 16, 2020.
- Chan DG, et al. Clinicopathologic study of conjunctivochalasis. Cornea. 2005;24:634.
- Watanabe A, et al. Clinicopathologic study of conjunctivochalasis. Cornea. 2004;23:294–298.
- Huang Y, et al. Conjunctivochalasis interferes with tear flow from fornix to tear meniscus. Ophthalmology. 2013;120:1681–1687.
- Holland E, et al. Ocular Surface Disease: Cornea, Conjunctiva and Tear Film. 2013. Saunders Elsevier.
- Doss LR, et al. Paste-pinch-cut conjunctivoplasty: subconjunctival fibrin sealant injection in the repair of conjunctivochalasis. Cornea. 2012;31:959–962.
Relevant disclosures
Desai: Bio-Tissue
Holland: None
Hovanesian: Katena
Salinger: Bio-Tissue
Trinh: None
Contact
Desai: desaivision2020@gmail.com
Holland: eholland@holprovision.com
Hovanesian: johnhova@gmail.com
Salinger: drsalinger@comcast.net
Trinh: tanya.trinh@gmail.com



