Glaucoma
September 2021
by Ellen Stodola
Editorial Co-Director
Though the trabeculectomy procedure is more than 50 years old, it is still considered to be the gold standard in glaucoma surgery. Even with new devices and techniques, particularly many microinvasive options, trabeculectomy is able to produce the best pressure-lowering effect.
Leon Herndon Jr., MD, and Douglas Rhee, MD, discussed the history of trabeculectomy, how it has evolved, and how it fits into the glaucoma treatment paradigm.
Dr. Herndon said he thinks trabeculectomy is still the gold standard of glaucoma surgery. “If you need a low pressure, there’s nothing that comes close to the lowering effect of trabeculectomy,” he said.

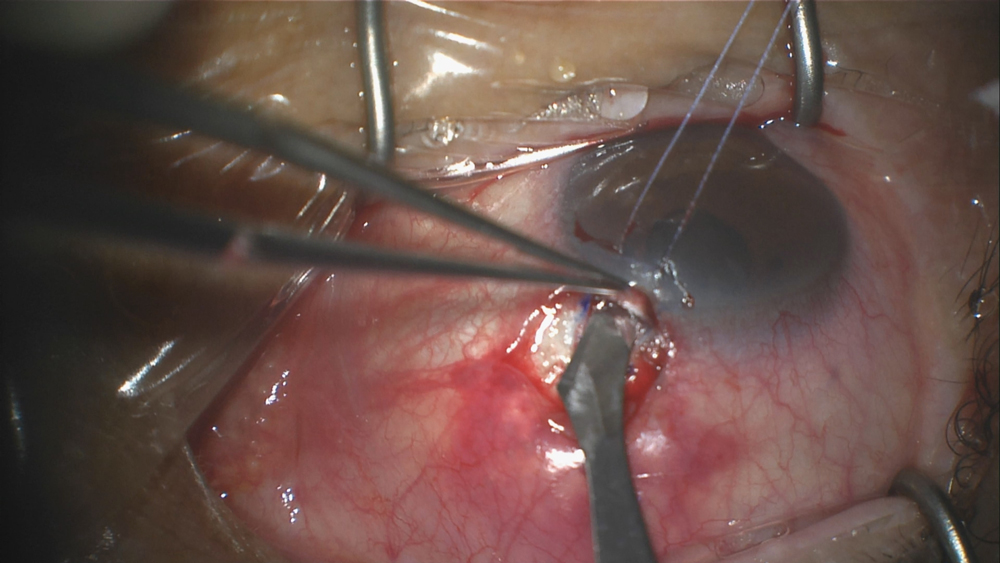


Source (all): Leon Herndon, MD
According to Dr. Rhee, the procedure is attributed to H. Saul Sugar, MD. Though he noted that the concept of having an open hole in the eye to drain fluid has been around since 1830, Dr. Sugar wrote about a progenitor of modern trabeculectomy in 1961,1 and J.E. Cairns, FRCS, later published on the method and reported on a guarded filtration procedure in 1968.2
Dr. Cairns popularized trabeculectomy, Dr. Herndon said. Before this, there were full thickness procedures, essentially making a hole in the eye with no cover. “Dr. Cairns decided to make a guarded trabeculectomy where you create a flap instead of just making the punch,” he said. “At the time there were so many complications with full thickness procedures, cataract formation, hypotony, etc., the guarded filtration procedures became more popular because of the greater safety profile.”
Evolution in technique
Dr. Herndon and Dr. Rhee agreed that though there has been some slight adjustments to the technique, there hasn’t been much evolution in the procedure as it was initially presented.
The main evolution, Dr. Herndon said, has been with antimetabolites and different techniques of applying mitomycin-C. He also mentioned how the technique has evolved for conjunctival dissection from limbal-based to fornix-based, the latter of which is more popular now.
“What we do now isn’t exactly what was initially published/studied, but it closely resembles it,” Dr. Rhee said. He added that in the 1970s and 1980s, there was some experimentation with different shapes and sizes of flaps, but it was determined that this didn’t make much of a difference.
What did make a difference, he said, was in the early 1980s, when Heuer et al. published the 5-FU trial of the first antimetabolite, which was designed to inhibit scarring and improve the survivability of the trabeculectomy.3
The next big advent, he said, was the use of mitomycin-C, credited to Chen et al.4 and Kitazawa et al.5 Dosing and timing of mitomycin-C has continued to be studied over the years.
Finally, Dr. Rhee mentioned the evolution of fornix-based flaps. Prior to this, physicians had been doing limbal-based flaps. Wells et al. published a study showing that fornix-based flaps do well,6 Dr. Rhee said. In modern trabeculectomy, the vast majority of glaucoma specialists use these, he said, but some still use limbal-based, which is a good option.
Gold standard despite other options
Dr. Herndon said he thinks trabeculectomy will be around for the foreseeable future until “we have a procedure that will get those trab-level pressures.”
“I’ve been doing this so long, and I wince when I see some patients on whom I [did trabeculectomy] 20 years ago who just had mild disease and they have huge blebs that are causing irritation, leaking, and potentially infection,” he said. “I would not recommend trab for mild to moderate disease at this point until you try something less invasive first.”
Still, Dr. Herndon doesn’t see the procedure going away. He said when the EX-PRESS Glaucoma Filtration Device (Alcon) came on the market, this helped take trabeculectomy to the next level.
Dr. Herndon is excited about the PRESERFLO MicroShunt (Santen), though he noted the data haven’t shown the same pressure-lowering effects as trabeculectomy.
Dr. Rhee agreed with Dr. Herndon that there is still nothing that can lower pressure as well as trabeculectomy. “We don’t have anything that’s as modifiable in the postop period,” he added. The other options are to wait and see or add glaucoma medications.
The only other procedure that offers the ability to modify it postoperatively is deep sclerectomy, Dr. Rhee said, where you can laser open Descemet’s window. But with trabeculectomy, there are things physicians can do to modify the wound healing response.
“Trabeculectomy has a lot of features that we wish we could change, but to date nothing has come along to unseat it as the gold standard,” Dr. Rhee said.
The closest thing is tubes shunts, but even these have not been shown to be superior to trabeculectomy.7
“Just because it’s the gold standard doesn’t mean that it’s always the first-line procedure,” Dr. Rhee said. “It depends on the patient’s individual need.”
Trabeculectomy may be the most effective procedure, but it’s certainly not the safest, he continued. In the appropriate situation, you still might do trabeculectomy first. It might be a good first-line approach for those who need very low target pressures.
He also mentioned the EX-PRESS Glaucoma Filtration Device, which he said is recognized as its own procedure with its own billing code, though there is some debate if it is truly unique in its mechanism or if it is an enhancement for trabeculectomy. “You do a trab, but instead of making a hole in the iridectomy, you put in an EX-PRESS shunt, and everything else is like a trab,” he said.
Dr. Rhee also mentioned PRESERFLO and the XEN Gel Stent (Allergan) as potential options, but he again reiterated the 50-year history of positive pressure-lowering results with trabeculectomy.
About the physicians
Leon Herndon Jr., MD
Duke University
Durham, North Carolina
Douglas Rhee, MD
Professor and Chair
Department of Ophthalmology and Visual Sciences
Case Western Reserve University
Cleveland, Ohio
References
- Sugar HS. Experimental trabeculectomy in glaucoma. Am J Ophthalmol. 1961;51:623–627.
- Cairns JE. Trabeculectomy: Preliminary report of a new method. Am J Ophthalmol. 1968;66:673–679.
- Heuer DK, et al. 5-fluorouracil and glaucoma filtering surgery. II. A pilot study. Ophthalmology. 1984;91:384–394.
- Chen CW, et al. Trabeculectomy with simultaneous topical application of mitomycin-C in refractory glaucoma. J Ocul Pharmacol. 1990;6:175–182.
- Kitazawa Y, et al. Trabeculectomy with mitomycin. A comparative study with fluorouracil. Arch Ophthalmol. 1991;109:1693–1698.
- Wells AP, et al. Cystic bleb formation and related complications in limbus- versus fornix-based conjunctival flaps in pediatric and young adult trabeculectomy with mitomycin C. Ophthalmology. 2003;110:2192–2197.
- Gedde SJ, et al. Treatment outcomes in the Primary Tube Versus Trabeculectomy Study after 3 years of follow-up. Ophthalmology. 2020;127:333–345.
Relevant disclosures
Herndon: Alcon
Rhee: Glaukos, Ivantis
Contact
Herndon: leon.herndon@duke.edu
Rhee: dougrhee@aol.com



