Glaucoma
December 2020
by Liz Hillman
Editorial Co-Director
Depending on what you define as a microinvasive glaucoma surgery (MIGS), you might think it first became available several decades ago with endocyclophotocoagulation (ECP), but many define the MIGS era beginning with the iStent (Glaukos), the first ab interno trabecular microbypass device approved by the FDA in 2012.
Since then there has been a steady stream of new devices and procedures classified as MIGS that have entered the market, and some are still in development. Though nearly a decade has passed since the more formal MIGS era began, are there still hurdles facing the IOP-lowering procedures?
According to three glaucoma specialists EyeWorld spoke with, the short answer is yes.
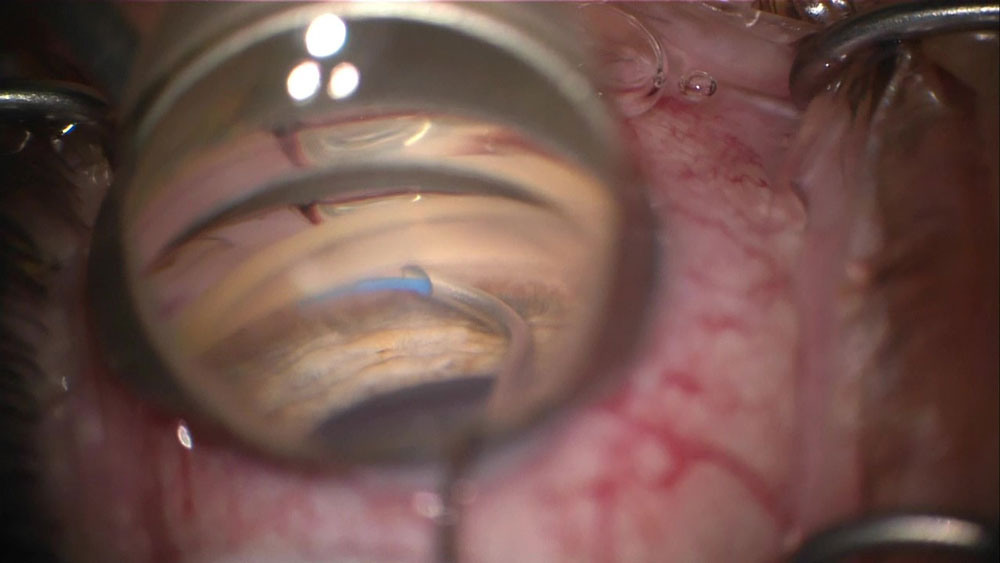
Source: Linda Huang, MD
1. Comparing it to trabeculectomy
Amy Zhang, MD, said one major hurdle is that MIGS are often still compared to trabeculectomy.
“Some say MIGS would be a replacement for trabeculectomy. I don’t think that should be the approach one takes with MIGS. I think it should be thought of as a bridge to possibly better IOP control,” she said. “I don’t think the gold standard in terms of trabeculectomy pressure lowering can be replaced by one MIGS device. That’s one of the biggest challenges, understanding where MIGS would fit in.”
2. Surgeon adoption
Thomas Patrianakos, DO, thinks the biggest hurdle facing MIGS is still surgeon comfort.
“Just like with any new procedure that’s out there, there’s a learning curve, and there will be complications that occur,” he said, explaining that the perception of getting over that learning curve and handling complications is still needed for MIGS acceptance by surgeons.
He also advised surgeons to not be put off by early complications.
“Reach out to colleagues doing the procedures, and you’ll be surprised that they probably had that same complications happen,” he said.
3. Approved for specific indications
Linda Huang, MD, addressed the hurdle of many MIGS being approved by the FDA for only certain types or severities of glaucoma and/or in combination with cataract surgery.
“This may limit the use of certain types of procedures even though patients may still benefit from them. For example, iStent or Hydrus [Ivantis] is not approved in patients who are pseudophakic, even if the device may be effective in lowering the patient’s pressure,” Dr. Huang said.
4. The data
All three doctors said when new devices and procedures are introduced, there are always safety and efficacy concerns until long-term data shows otherwise.
“Certain MIGS devices have been approved for some time and have had longer follow-up times. It is always important to continue to monitor and assess patients for safety and efficacy of a device,” Dr. Huang said.
Dr. Zhang said she thinks many physicians don’t think they have adequate long-term data for more modern MIGS.
“Someone opposed to MIGS might say ‘Look at CyPass,’” Dr. Zhang said, referencing the recall of Alcon’s suprachoroidal stent in August 2018. A 5-year post-surgery data study found the potential for endothelial cell density loss if too much of the device extended into the anterior chamber.
Dr. Patrianakos brought up another data concern. There are different study designs, different definitions of success, some use washout periods and some don’t, different years of follow-up, and different experience levels by the surgeons involved in the studies.
“One of the things we need to do to solidify MIGS as a procedure is plan for these future studies to be more standardized and make comparisons between studies easier and also compare to traditional glaucoma therapies,” Dr. Patrianakos said.
5. Intraoperative gonioscopy
Learning intraoperative gonioscopy is essential for most MIGS procedures.
“It’s important if you’re going to do any of this that you’re comfortable with intraoperative gonioscopy,” Dr. Patrianakos said.
Dr. Zhang advised ophthalmologists to start practicing visualization of the angle through intraoperative gonioscopy on all of their standard cataract surgeries.
6. Financial hesitations
Equipment concerns could be a barrier to some physicians bringing certain MIGS options into their practice. Some MIGS are only single-use, single-packs, Dr. Zhang said, while others require a unit to be purchased for multiple uses.
Some MIGS are also less likely to be covered by insurance compared to traditional glaucoma surgery, according to Dr. Huang.
Dr. Zhang said she doesn’t think patient perception is too much of a barrier to MIGS. In her practice, if she recommends a MIGS procedure, patients are usually on board. She said she sets honest expectations for them, explaining that they might not take the patient completely off medications but could reduce the medication burden. In addition to potentially lowering the amount of drops needed, Dr. Zhang said the visual outcomes of phaco combined with a MIGS procedure are better than phaco combined with trabeculectomy. What’s more, cataract surgery causes inflammation and can cause a trabeculectomy to fail when done in combination.
“When you do MIGS with cataract surgery, it tends to have a better outcome visual outcome than phaco plus trabeculectomy,” Dr. Zhang said.
ARTICLE SIDEBAR
Glaucoma pipeline update
Dr. Huang gave a quick update on what’s in the pipeline for glaucoma that she’s looking forward to. PRESERFLO (Santen, formerly the InnFocus Microshunt), an ab externo subconjunctival MIGS similar to the XEN Gel Stent (Allergan), is anticipated. The iStent infinite (Glaukos), which Dr. Huang said will have three stents in a standalone procedure for severe and refractory glaucoma, is also expected. Additionally, there are some drug-eluting implantable devices that may benefit glaucoma patients in the future, she said.
About the doctors
Linda Huang, MD
Glaucoma Institute of Northern New Jersey
Rochelle Park, New Jersey
Thomas Patrianakos, DO
Cook County Health
Northwest Chicago Eye Specialists
Chicago, Illinois
Amy Zhang, MD
Assistant Professor of Ophthalmology
Kellogg Eye Center
University of Michigan
Ann Arbor, Michigan
Relevant disclosures
Huang: Sight Sciences
Patrianakos: None
Zhang: None
Contact
Huang: lindayhuangmd@gmail.com
Patrianakos: tpatrianakos@yahoo.com
Zhang: amydz.@med.umich.edu


