News & Opinion: Anterior segment grand rounds (ASGR)
April 2016
By Steven Safran, MD

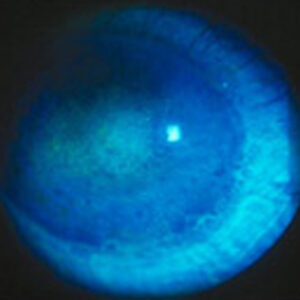
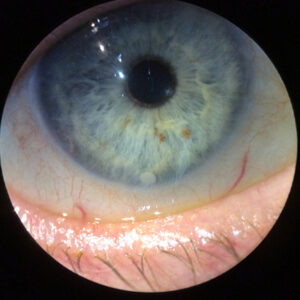
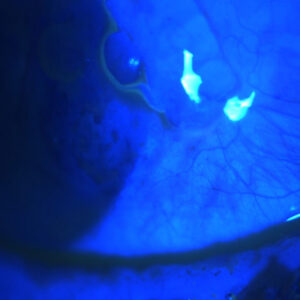
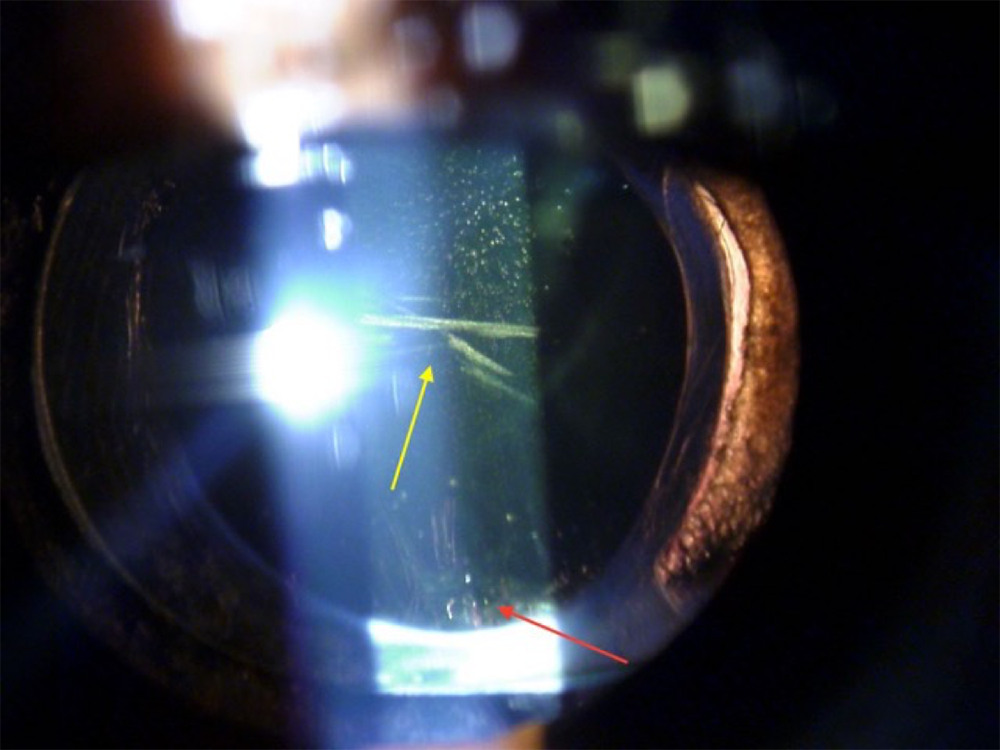
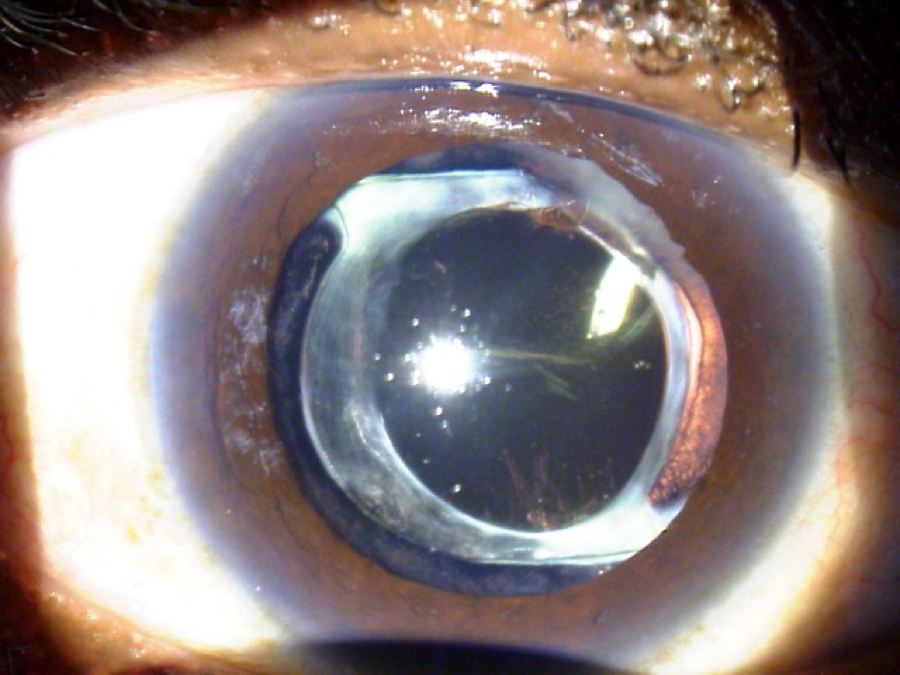
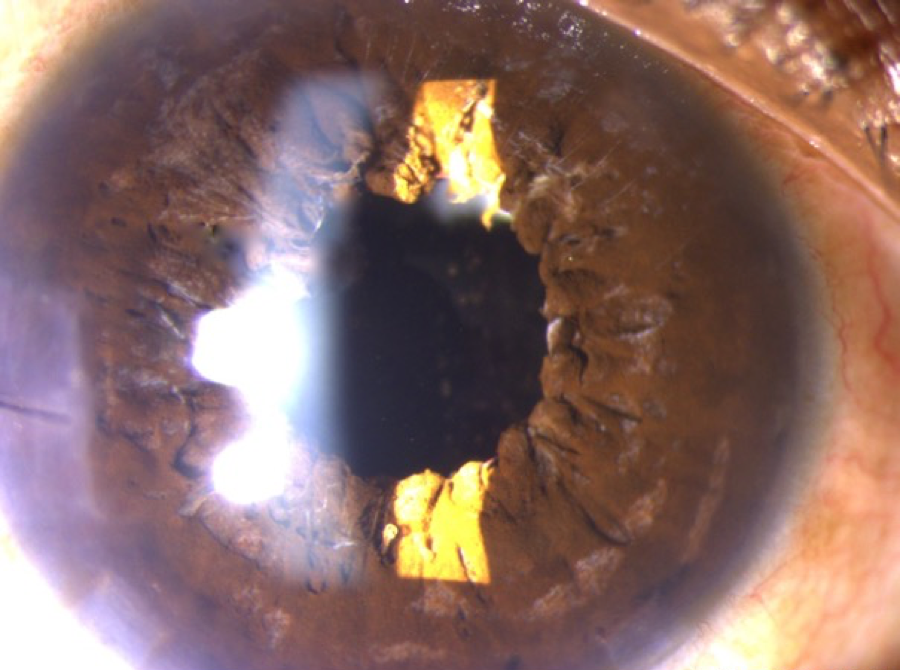
This is a 55-year-old active male who had blunt trauma to the OD. He developed a traumatic cataract and subsequently had cataract surgery. Since the surgery, however, he has been bothered by intractable glare in this, his dominant right eye. He was referred to me for an opinion on what can be done to fix his glare problem. His refractive outcome in this eye is +1.5. The other eye is phakic and plano. On exam the eye has a fixed and dilated pupil. The images included have been taken without dilating drops placed in the eye. His pupil is fixed in this position and does not budge with bright light or pilocarpine. He has an AcrySof lens (Alcon, Fort Worth, Texas) with a series of smudges or scratches centrally, moderate to severe glistenings in the optic, and he had extensive YAG capsulotomy treatment extending almost to the edge of the optic 360 degrees. On gonioscopy it can be seen that there is a diffuse, patchy loss of zonules, mostly associated with his blunt trauma and previous surgery. The patient’s best corrected vision in this OD (his dominant eye) is limited to 20/40 because of the macula damage associated with his trauma. He’s also very bothered by glare and light sensitivity.
—Steven Safran, MD, ASGR editor
Patient seeks to fix a glare problem after surgery
Eric Donnenfeld, MD, Rockville Centre, New York, said, “This patient has 3 significant problems that are all likely contributing to his problem of glare and halo: IOL opacifications, hyperopic refractive error, and a fixed dilated pupil. The cataract surgery was otherwise done well and the 1-piece acrylic IOL is in the bag. The decision tree should be based on which of the problems is most contributing to his poor quality of vision and then developing a treatment plan based on risk and reward. An IOL exchange is the obvious first solution, but the trauma and zonular weakness, open posterior capsule, and IOL firmly adherent to the capsular bag make IOL exchange the highest risk procedure.
“I would begin by giving the patient a +l.5 D cosmetic contact lens with a normal-sized pupil that resolved the issue of the fixed iris. This would resolve 2 of the 3 problems and would allow the surgeon to assess the contribution of these issues to the patient’s symptomatology. If the cosmetic contact lens significantly resolved the patient’s glare and halo, he could be offered this treatment as a permanent solution. If a contact lens was not the patient’s treatment of choice, a purse string iridoplasty to bring the pupil down to a normal size or an artificial iris would be excellent choices. While the surgeon was in the eye, the ‘scratches’ could be assessed and if possible polished and resolved. LASIK or PRK at a later date could resolve the residual refractive error.
“If the cosmetic contact lens does not resolve the patient’s symptoms, after an extensive informed consent, I would perform an IOL exchange, carefully opening up the capsular bag with dispersive viscoelastic on a 30-gauge needle, placing viscoelastic behind the IOL to tamponade the vitreous face, and placing the appropriate power, zero aberration 3-piece IOL behind the original IOL prior to bisecting the acrylic IOL and removing it from the eye. The new IOL could then be placed in the sulcus and centered with a posterior capture. The purse string iridoplasty would bring the pupil down nicely.”
David Chang, MD, Los Altos, California, said, “Differentiating whether the intractable glare is due to the traumatic mydriasis or the optic scratches is crucial. The scratches would likely cause specific symptoms of radiating lines from point sources of light. Trying a painted contact lens might be useful. If this significantly improved his symptoms, it would argue for doing an iris suture cerclage procedure. Two oppositely placed interrupted 10-0 Prolene sutures at the pupil margin will create a nicely rounded smaller pupil. Exchanging the IOL prior to iris suturing is possible. Although it would likely entail an anterior vitrectomy, there is a good anterior capsular platform to fixate a 3-piece IOL in the sulcus. An additional benefit might be improvement of his refractive error and anisometropia. The main danger would be further capsular dehiscence due to the traumatic zonulopathy, and after dissecting the optic free, the haptics should be amputated and left behind due to fibrosis around the bulbous haptic tip. Whether or not to exchange the IOL would depend on determining whether the optic scratches are causing severe enough radiating glare streaks.”
Michael Sulewski, MD, Philadelphia, noted, “This was the patient’s dominant eye, but due to permanent macular damage and best corrected vision of only 20/40, this eye will no longer be the dominant eye, and this patient is relatively functionally monocular. I think his most compelling problem is the intractable glare, as the visual acuity will always be limited compared to the other eye, however, the glare will affect his overall binocular function. Even though there are some blemishes on the IOL, and some degree of zonular damage, the IOL looks perfectly centered and there is no apparent pseudophakodonesis. Therefore, I would be inclined to leave the IOL alone at this point. I would try to fit this patient with a contact lens with shading and with the +1.5 refractive correction. If the patient is unable to tolerate the contact lens or if the glare symptoms are not improved to his satisfaction, then surgery is indicated.
“I would concentrate on addressing the glare issue by suturing the mydriatic pupil using either the sliding Siepser knot technique, the cerclage technique or the modified McCannel suturing method. The other possible option would be to use an artificial iris implant. I am not as concerned with the residual +1.5 postop refractive surprise as that could be handled with PRK or LASIK if necessary, and if you do an IOL exchange with an anterior or pars plana vitrectomy, there is no guarantee that you will hit the refractive mark as we can’t always ensure where the effective IOL position will end up. Also, since the patient is functionally monocular with the macular scar, I don’t have a problem asking him to wear polycarbonate glasses with the +1.5 lens OD and plano OS since he should have protection for the healthy OS. He also needs to wear glasses anyway for reading. He is only 55 years old and I would not be in a hurry to suture or glue in another IOL now in anticipation of a future dislocation that may or may not happen. The long-term stability of fixating the haptics by sutured-in or glued methods into a scleral groove is not known.”
Uday Devgan, MD, Los Angeles, commented, “I would approach this case in a step-wise pattern to find the least invasive remedy. The first step is determining whether he has symptoms other than intractable glare, which is likely due to the chronic mydriasis.
“Specialty cosmetic contact lenses are available with a small central aperture to give an effective pupil size of 3 mm or so. This could also be ordered in the +1.5 D strength in order to correct the refractive error at the same time. Should this contact lens solve the majority of the patient’s problems, further surgery may not be required.
“If the contact lens solves the glare issue but the patient does not desire to wear them daily, a purse string suture can be placed in the iris to bring the pupil size down. The ideal balance is a pupil size of about 3.5 mm, which would still enable a view of the retina while decreasing glare. This purse string suture would only resolve the mydriasis, and the patient would still require spectacles for the +1.5 D of hyperopia.
“The last option, and most invasive one, would be an IOL exchange with the pupilloplasty. Despite having glistenings and linear marks on the central optic, these may not induce much, if any, perceptible dysphotopsia.
“Due to the size of the posterior capsulotomy and area of zonular loss, this has a high risk of vitreous prolapse, which would require an anterior vitrectomy and possible fixation of the IOL. With the iris issues that are pre-existing, suturing an IOL to the back of the iris is not a great choice. This means that the Agarwal ‘glued IOL’ method of intrascleral haptic fixation would be a better choice. Such a surgery involving the IOL explantation, anterior vitrectomy, IOL scleral fixation, and purse string pupilloplasty is complex and carries a higher risk than the other options. The patient should be warned that there is a chance he could be trading in tolerable vision for no vision.”
Source all: Steven Safran, MD
What was done
The consultants bring up many points that I considered. I did not spend time experimenting with contact lenses because the patient was traveling from a distance and was more interested in an immediate surgical solution to the problem. I felt the dilated pupil and the scratched lens were issues causing problems and decided it would be best to fix both with 1 procedure. If I chose to do an iris cerclage and he was not happy, I’d have boxed in the old IOL and that would be checkmate. I decided to perform a combined IOL exchange for a 3-piece silicone lens that was optic captured in the rhexis, pars plana vitrectomy and iris cerclage. The patient ended up plano-0.25 x 180 and had 1 line of improvement in his best corrected visual acuity. He was very happy with the visual outcome but even more so with the cosmetic outcome as he always hated the way his eye looked with the fixed dilated pupil.
Contact information
Chang: dceye@earthlink.net
Devgan: devgan@gmail.com
Donnenfeld: ericdonnenfeld@gmail.com
Safran: safran12@comcast.net
Sulewski: Michael.Sulewski@uphs.upenn.edu