Cover Feature: Refractive
March 2012
by Faith A. Hayden
EyeWorld Staff Writer
What can be done for patients with post-LASIK corneal neuralgia?
A 30-something female with a history of bilateral, uncomplicated LASIK 2 years prior comes into your office complaining of persistent burning pain, almost a foreign-body sensation in both eyes. A simple breeze across her face is excruciating. The pain is so severe it prevents her from living a normal life, and she has thoughts of suicide. The slit lamp examination, though, is overwhelmingly unremarkable and free of corneal staining. Maybe she has slightly variable tear function or reduced tear break-up time, but there’s nothing to warrant her extreme symptoms.
“Patients go to their ophthalmologists, some of them suicidal because of the pain, and their eyes on the slit lamp look perfectly normal,” said Perry Rosenthal, M.D., founder, Boston Foundation for Sight. “Doctors send them to a psychiatrist because they think the [patients are] exaggerating. It just adds to the patients’ burden.”
Before you dismiss this patient as a crazy hypochondriac and send her on her way, consider corneal neuropathic disease, an extremely rare condition that causes intense pain along corneal nerves.
“The hallmark of this disease is how uncomfortable patients are. These patients are very difficult to treat and keep coming back to your clinic, failing all the therapies you give them,” said LCDR John B. Cason, M.D., cornea, external disease, and refractive surgery, Naval Medical Center, San Diego, during the 6th Annual International Military Refractive Surgery Symposium held in San Antonio in early January. “Because of that, many of us think they’re just making it up. These patients have a true disease process, it’s just not well understood.”
What causes corneal neuralgia?
No one knows exactly what causes this neuropathic pain to develop after photorefractive keratectomy (PRK) and LASIK, but there are some theories. First, it’s important to note that the cornea is the most powerful pain generator in the human body, 200 times more powerful than skin.
“The most common cause of neuropathic pain anywhere in the body is damage to the sensory nerves,” Dr. Rosenthal said. “Obviously, LASIK and PRK are classic examples of this. It’s what happens next after the damage that determines if the post-op pain resolves as the corneal tissue heals or whether it triggers the development of that chronic disease called neuropathic pain.”
The pain becomes chronic when it’s centralized and in the brain, which is called central sensitization. It’s when the central sensitization is no longer reversible that it’s neuropathic.
“In a simple way, acute pain can in certain vulnerable people damage their pain system. And the pain continues independently of initial trauma or insult,” Dr. Rosenthal explained. “So for example, corneas can heal perfectly fine and normal. But you can’t see the nerve circuitry. The ophthalmologist just assumes if you can’t see it, it isn’t there. This is wrong. If a patient has chronic pain and you can’t see it, it’s neuropathic pain unless proven otherwise.”
Diagnosing the pain
Patients with corneal neuralgia may complain of burning, stinging, scratchiness, or something as vague as pure pain. The first step toward a diagnosis is differentiating between discomfort from dry eye, blepharitis, and corneal pain.
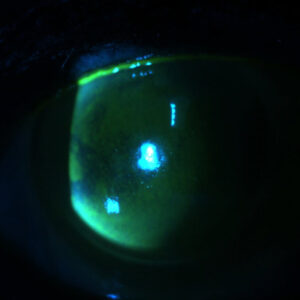
“There’s a continuum of disease that’s partially due to the dry eyes patients develop after refractive surgery and partially due to inflammation, which is leading to the corneal neuralgia,” explained Pedram Hamrah, M.D., director, Ocular Surface Imaging Center, Henry Allen Cornea Scholar, Cornea & Refractive SurgeryService, Massachusetts Eye & Ear Infirmary, Boston. “In dry eyes, you can obviously see the surface staining and other dry eye signs. In corneal neuralgia alone, you don’t see these signs. It’s just the symptoms of the patient.”
A simple slit lamp examination is not enough to diagnosis this condition, Dr. Hamrah said. You must examine these patients on a cellular level with an in vivo confocal microscope. Using this, “you can see inflammation lingering,” he said. “You can see abnormalities of the nerves. There are things we can detect on a pathological level, but not at the slit lamp level necessarily.”
Other telling symptoms include exaggerated pain response to touch, air, and drops; lowered Schirmer’s scores, but frequently borderline or within the normal range; and depressed cornea sensitivity by Cochet-Bonnet esthesiometry.
“There’s a high likelihood we’ve all seen patients like this and attributed it to something else,” Dr. Cason said. If patients aren’t responding to dry eye treatments such as artificial tears and anti-inflammatories, he said, “our suspicion has to be high.”
A multidisciplinary treatment plan
Depending on the disease stage, patients with corneal neuralgia may need special, usually multifaceted, treatment. If caught and treated early, patients respond fairly well.
“When I am referred [patients] 2-3 months after LASIK and they have pain, almost all of them have lingering inflammation,” Dr. Hamrah said. When treated, the neuralgia goes away. However, “if the patient has had this for 6 months to a year, that becomes difficult to treat,” he said.
Dr. Rosenthal agreed that central sensitization could be avoided if the pain is treated early.
“I theorize that if we limit the pain and enhance the healing of the nerves and the corneal epithelium, theoretically this devastating centralized pain may be aborted,” Dr. Rosenthal said. “I think there’s a chance of developing that type of intervention.”
For advanced disease, Dr. Cason recommended treating the dry eye conditions with lubrication, anticonvulsants, tricyclic antidepressants and serotonin reuptake inhibitors, and the scleral reservoir lens and evaporation-prevention goggles. The problem with the scleral lens is some patients have sensitivity in the conjunctiva and may feel the lens under their eyelid.
“Despite the fact that the cornea is completely bathed in fluid, they still have pain sensation,” he explained. “Unfortunately, a lot of these patients aren’t helped by this.”
Dr. Hamrah has had some success with autologous serum tears (AST), which promote nerve regeneration. AST can be problematic to prescribe though, as not all compounding pharmacies make it.
“If the pain has shifted toward the brain and there’s a central sensitization, you have to co-manage these patients with neurologists or pain specialists,” Dr. Hamrah said. “They have a variety of things [from] systemic medication to nerve blockers to acupuncture.”
Preventive screening
A key to understanding corneal neuralgia and preventing it from occurring in the first place is identifying the patients at risk.
“I strongly believe that one of the significant risk factors is autoimmune disease,” Dr. Rosenthal said.
Diseases to screen for include Sjogren’s syndrome, fibromyalgia, chronic interstitial cystitis, irritable bowel syndrome, chronic fatigue syndrome, and multiple chemical hypersensitivities.
“One of the important parts in getting patient history is detailing any possible symptoms of autoimmune disease such as dry mouth. Go down the whole list,” Dr. Rosenthal said. “Is there family history of neuropathic pain elsewhere in the body?”
In that case, one has to ask, should systemic pain disorders be a contraindication to refractive surgery?
“Yes,” Dr. Rosenthal said. “Laser keratorefractive surgery is not treating a disease. If you’re dealing with a healthy tissue, then the complication rate should be zero. I’m sure this would exclude many people who could have done well. But patients should at least know about this risk. I’d say 90% of my [neuralgia] patients have thoughts of suicide. Just imagine, you open your eyes in the morning and you know the whole day you’re going to have tremendous pain. The despair is incredible.”
Although this disease can be debilitating, it’s important to stress its rarity. Some patients with autoimmune disease may develop corneal neuralgia, but certainly not all. Corneal neuralgia may need further study before refractive surgeons begin to list autoimmune disease as a decisive contraindication for surgery. We do know enough about the disease, however, to say with absolute certainty that these patients aren’t crazy.
“The most important thing is these patients aren’t dismissed,” Dr. Hamrah said. “Just because you can’t see it on the slit lamp doesn’t mean it’s not there. It’s important, if [patients have] symptoms, to send them to centers that have the capability of analyzing them further instead of just telling [them], ‘It’s nothing.'”
ARTICLE SIDEBAR
Tricks for avoiding intraoperative ingrowth
- In keeping ingrowth at bay, Dr. Desai suggested the following:
- Avoid giving the patient too many anesthetic drops
- Make sure that the anesthetized patient is not sitting around for long periods before treatment
- If there’s an epithelial abrasion at the flap edge, brush the epithelium back and place a contact lens
- Irrigate just the right amount, making sure that there are no cells underneath the flap or at the edges, but not so much as to swell or thicken the flap
- After the flap is down, squeegee any fluid toward the edge to maximize flap adherence
Editors’ note
The doctors mentioned have no financial interests related to this article.
Contact information
Cason: john.cason@med.navy.mil
Hamrah: pedram_hamrah@meei.harvard.edu
Rosenthal: perry.rosenthal@comcast.net