Cataract: YES Connect
November 2016
by Liz Hillman
EyeWorld Staff Writer

Long eyes can present their own specific challenges before, during, and after cataract surgery. For example, a predisposition to retinal tear and detachment requires heightened concern both preoperatively and postoperatively. Ocular biometry and intraocular lens power selection carries its own inherent pitfalls in these patients. During surgery, reverse pupillary block and weak zonular support of the capsular bag may need to be specifically acknowledged and addressed.
In this month’s column, we call upon the expertise of John Berdahl, MD, Jessica Ciralsky, MD, and Zaina Al-Mohtaseb, MD. They discuss their approach to surmounting these challenges. In addition, they share at what axial length they start to modify their approach, under what circumstances they might involve their posterior segment colleagues, and how they set expectations for patients regarding postoperative refractive outcomes.
One additional pearl: To avoid reverse pupillary block, a simple tip shared with me by Robert Cionni, MD, is to enter the eye with infusion off, place a second instrument or the handpiece tip between the posterior iris and anterior capsule, and then turn on infusion by depressing the foot pedal to position one (not two or three). This maneuver avoids reverse pupillary block altogether.
—Charles Weber, MD, YES Connect co-editor
Meeting the challenges that come with eyes of long axial lengths
Just as eyes with short axial lengths come with their own set of preop, perioperative, and postop pearls— as discussed in the “YES Connect” column in the October issue of EyeWorld—eyes with long axial lengths also have special considerations for cataract surgery.
Just what is a long eye? Each surgeon has a slightly different benchmark. John Berdahl, MD, Vance Thompson Vision, Sioux Falls, South Dakota, said he gives specialized attention to eyes as they start measuring 28 mm or greater in axial length. Jessica Ciralsky, MD, assistant professor of ophthalmology, Weill Cornell Medical College, New York, said she’ll start altering her decision-making regarding biometry in eyes greater than 26 mm.
Preoperative exam
A peripheral retinal exam is imperative for patients with long axial lengths. If peripheral retinal pathology is found, Drs. Berdahl and Ciralsky said they would bring in a retinal specialist for his or her opinion prior to cataract surgery.
“That’s particularly true because we do intravitreal injections. … Because we are putting something in the vitreous, it’s ideal to have retinal input sometimes,” Dr. Berdahl said.
Zaina Al-Mohtaseb, MD, assistant professor, Baylor College of Medicine, Houston, said within the last few months she and her colleagues have been obtaining OCT images of maculas preoperatively, in addition to a dilated retina exam, on all of their cataract patients.
“We are placing more premium lenses, including low add multifocals … and extended depth of focus and toric IOLs,” she said. “We want to diagnose any subtle retinal abnormality, such as drusen or ERMs [epiretinal membranes], to avoid putting premium lenses in, since blurry vision, glare, and halos can be magnified in these situations, and to discuss postoperative outcome expectations.”
Dr. Al-Mohtaseb said she doesn’t get a retina specialist involved in all of her highly myopic cases, but if she diagnoses ERM, macular edema, lattice, or retina tears, for example, she will. The risk of retinal detachments or tears after cataract surgery is higher in myopic patients and that is important to discuss with them, she said.
“I think that it’s a comfort level. If you feel comfortable with your peripheral retinal exam and you’re treating the patient the way you would treat your mother if she was your patient, then I think you’re good to go,” Dr. Berdahl said. “But if it was your mom and you would get a peripheral retinal exam by a retinal specialist, then you should. It’s one of the best questions we can ask ourselves: What would I do if this was my mom?”
Dr. Al-Mohtaseb also noted that optical biometry is more accurate than ultrasound at measuring axial length in these patients because it measures to the fovea, not a possible posterior staphyloma. Drs. Berdahl and Ciralsky said they’d prefer optical biometry to measure length as well.

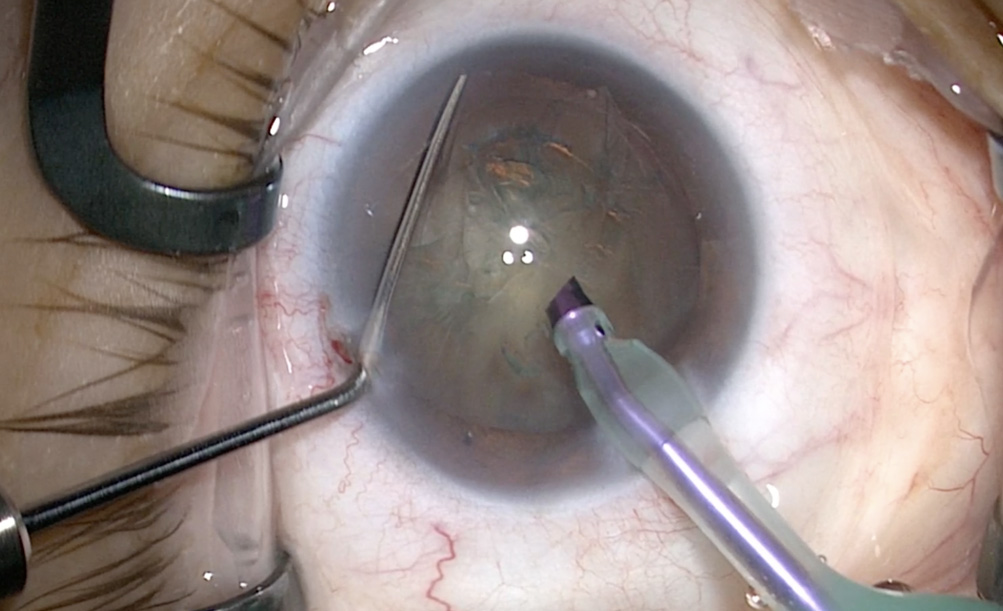
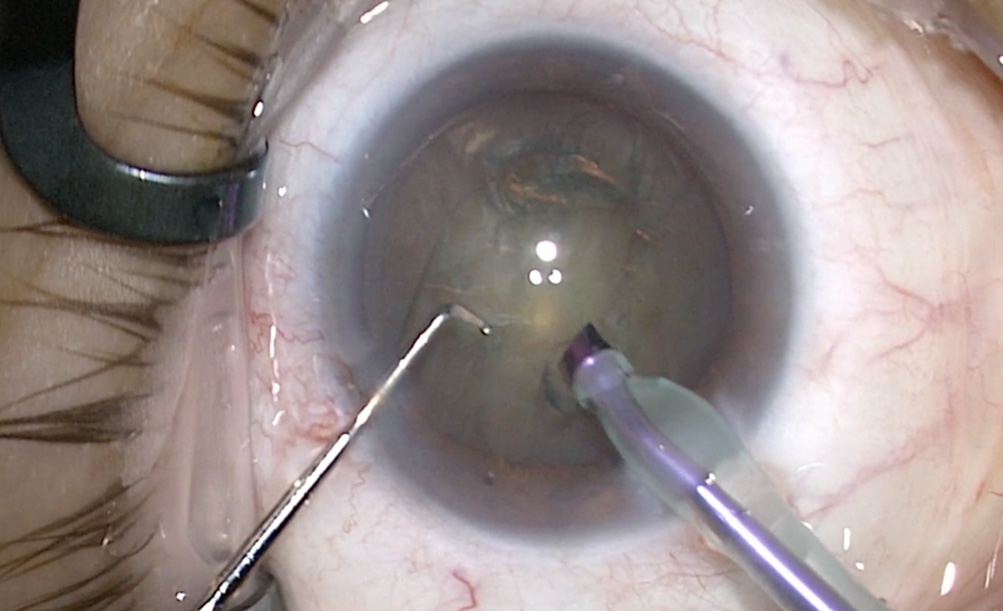
Source: Zaina Al-Mohtaseb, MD
Intraoperative challenges
While having a larger anterior chamber depth makes cataract surgery easier than if it were small, as in hyperopic eyes, Dr. Al-Mohtaseb said complications such as reverse pupillary block or lens/iris diaphragm retropulsion syndrome can occur, especially in post-vitrectomy patients.
In the event of a pupillary block, a second instrument can lift the iris off the capsule to allow fluid to circulate back to the posterior chamber and return the iris/lens diaphragm to its normal position, Dr. Al-Mohtaseb said. But the issue is the pupil can be smaller after this happens. “It’s best to avoid this from occurring instead of dealing with it when it occurs,” she said. “I do not enter the wound irrigating—I am on foot position zero—since the anterior chamber is filled with OVD. I insert my phaco tip and then use my second instrument to lift up the iris before going to foot position two.”
Dr. Berdahl said physicians should not only prepare for the potential of a reverse pupillary block but for the eye to feel bouncier and the cataract softer than usual as well.
IOL calculations
IOL power formulas tend to select lower powers than needed for long eyes, resulting in hyperopic errors, Dr. Al-Mohtaseb said. As such, the axial length needs to be adjusted, rather than the lens constant, she explained, citing work by Douglas Koch, MD, and Li Wang, MD.
“For patients with axial lengths greater than 25.2 mm, which we consider long eyes, the Wang-Koch AL adjustment reduces the risk of these hyperopic errors,” Dr. Al-Mohtaseb said. “The AL optimization adjustment can be used with traditional formulas (Holladay 1, Haigis, SRK/T, Hoffer Q) and was found to result in less postoperative hyperopic surprise, especially in patients needing IOL powers less than 6 D.
“More recently, the Barrett Universal II formula, which is based on paraxial ray tracing, has also been shown to be very accurate in predicting IOL power in long eyes,” Dr. Al-Mohtaseb continued.
Dr. Ciralsky said she uses a traditional formula, typically the SRK/T formula with the Wang-Koch adjustment. Dr. Berdahl said he leans heavily toward the Barrett Universal I formula but does look at a number of formulas for these eyes.
“I’m hopeful that the Hill-Radial Basis Function (RBF) will make us even better at this,” Dr. Berdahl said, referencing the Hill-RBF Calculator, a tool available on the ASCRS website. “I also use intraoperative aberrometry; that’s my tie-breaker if a patient is looking to be spectacle independent. The challenge in these highly myopic eyes is getting them firm enough to get an accurate ORA [Alcon, Fort Worth, Texas] reading, which may take additional viscoelastic.”
Patient conversation
The conversation about expected outcomes needs to be tailored for these patients as well.
If the patient is highly myopic in both eyes but only has a cataract in one, that’s an important consideration.
“Are you going to condemn patients to high myopia for the rest of their life by leaving them myopic so they don’t develop anisometropia afterward? Are they going to tolerate a contact lens well in the other eye? Are you going to plan for cataract surgery in the second eye even though there may not be a cataract there yet? Those are important discussions,” Dr. Berdahl said.
In these cases, Dr. Berdahl said his preference is to shoot for plano or a little bit of myopia and see if they tolerate a contact lens. If they can’t, then he would perform a lens exchange or cataract surgery on the second eye.
Highly myopic cataract patients are also often on the younger side, which Dr. Berdahl pointed out means they have a lot to gain as much of their myopia could be fixed. At this point in their lives though, they’re often only in the early or mid-stages of presbyopia.
“You need to have a good conversation about what it means if you’re going to use a monofocal lens, that they’re not going to be able to read up close anymore,” he said. “For all of their lives, their safety blanket has been if they hold something right in front of their eyes, they can read it. That’s going to go away with cataract surgery.”
As such, Dr. Berdahl said you might have to set the expectation for spectacle dependence.
“If patients are expecting spectacle independence, let them know that there’s a decent chance they’ll need a LASIK enhancement or an IOL exchange afterward, but that you’ll do your best to try and accomplish it with the first surgery,” he said.
Dr. Ciralsky said due to the complications associated with cataract surgery in long eyes and the difficulty in IOL calculations, she would advise beginning surgeons to postpone these cases until they are more experienced.
Editors’ note
Dr. Berdahl has financial interests with Alcon, Abbott Medical Optics (Abbott Park, Illinois), and Bausch + Lomb (Bridgewater, New Jersey). Drs. Ciralsky and Al-Mohtaseb have no financial interests related to their comments.
Contact information
Al-Mohtaseb: zaina@bcm.edu
Berdahl: john.berdahl@vancethompsonvision.com
Ciralsky: jessciralsky@gmail.com