Refractive
March 2021
by Ellen Stodola
Editorial Co-Director
When it comes to premium lenses, patients have high expectations for great outcomes. Neda Nikpoor, MD, Keith Walter, MD, and Blake Williamson, MD, discussed some of the technologies that they use preoperatively, intraoperatively, and postoperatively to help achieve excellent outcomes.
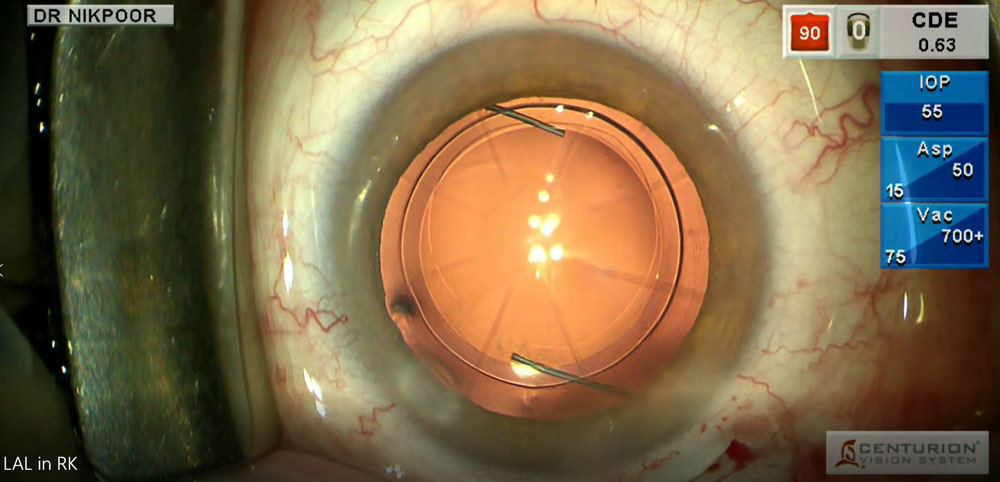
Source: Neda Nikpoor, MD
Preoperative technologies and testing
Dr. Nikpoor said that every patient who comes into her office for a refractive lens exchange (RLE) or cataract evaluation gets the same testing. This includes a preoperative macular OCT, topography, RNFL analysis, and aberrometry. She will also use the HD Analyzer (Keeler) on every patient, which she said helps by giving an objective assessment of the tear film. “Comparing this index with the iTrace Dysfunctional Lens Index [Tracey Technologies] helps me grade the impact of very early lens changes,” she said.
She noted that having a high-quality biometer is helpful for measuring posterior astigmatism; she uses the IOLMaster 700 (Carl Zeiss Meditec).
She will also obtain a LipiScan (Johnson & Johnson Vision) on every patient and likes to use epithelial mapping.
“We don’t use it on everyone, but we’ll use it if someone is post-refractive or if we think they have OSD or early keratoconus,” Dr. Nikpoor said.
This preoperative plan, Dr. Nikpoor said, is used for all cataract patients, even those getting standard IOLs. Additionally, for cataract patients getting premium lenses, she performs a standard OSD optimization protocol that includes warm compresses, lid scrubs, and artificial tears. She will add in more treatments as needed, including LipiFlow (Johnson & Johnson Vision) and/or pharmaceutical dry eye treatments.
Dr. Nikpoor said measurements used for the IOL calculation—topography, aberrometry, and IOLMaster—are repeated so there are two sets.
All of this information is consolidated into a grid with the astigmatism measurements.
Dr. Nikpoor said she uses VERACITY (Carl Zeiss Meditec) for all IOL calculations to help with IOL selection and finds it particularly useful for toric lenses because she can toggle between different measurements, toric calculators, and other data. She added that VERACITY is helpful for post-refractive cases, as it has a built-in calculator for that. She described it as a useful tool that moves everything from the EHR to the VERACITY system.
Dr. Williamson stressed the importance of having a healthy eye for advanced IOLs. He said the physician has to make sure they have all the testing in place to confirm it’s a pristine eye because these implants are very sensitive to any type of comorbidity or aberration.
He examines the ocular surface and may use point-of-care testing, such as the InflammaDry (Quidel) and TearLab Osmolarity Test (TearLab). He also mentioned doing meibography on the Keratograph (Oculus) if the meibomian glands are a concern.
“Everyone is going to get topography and tomography,” Dr. Williamson said. He also likes to get an OCT of the macula on every patient, regardless of what lens is being putting in.
Dr. Williamson will sometimes use the HD Analyzer preoperatively in less dense cataracts, which he said will give him an idea of the ocular scatter index when symptoms and complaints seem to outweigh the clinical exam. This device will also offer objective data on dry eye.
Dr. Walter said that he always uses the IOLMaster or LENSTAR (Haag-Streit) to get accurate measurements and calculations. “I only use the Barrett formulas, as they are the most accurate,” he added.
Dr. Walter will use macular OCT to look for any potential problems that might render the patient a non-candidate for a premium lens. “Corneal topography is also important especially with prior LASIK and to rule out bad ocular surfaces or other cornea disorders,” he said.
He added that he thinks that all of these technologies are “absolutely necessary, unless you have a patient with low cylinder, a great ocular surface, and no history of LASIK; then maybe you could skip the topography and just use the biometry to guide you,” he said.
Most important technologies
Dr. Walter said biometry is the standard of care and absolutely needs to be done. “The days of A-scans and manual Ks are over and are below the standard,” he said.
He added that “macular OCT has saved me so many times in picking up ERMs or macular holes that it must be done on every patient.” The last thing you want is to do a perfect surgery and the patient is unhappy because they can’t see, he said. They typically will think that you “caused” the problem, even though it was pre-existing.
Dr. Williamson said it’s possible that not all ophthalmologists have access to all the advanced technologies that he’s using. Most may just be getting a biometry, he said, and if concerned about something they see on the slit lamp exam, they probably have the capability to get an OCT. “I don’t know if we can say it’s standard of care to get a topography/OCT on every cataract patient. But I do think it should be simply because the OCT can see much finer details than the human eye at the slit lamp,” he said.
Intraoperative tools
Dr. Walter said he likes to use the CATALYS laser (Johnson & Johnson Vision) for his premium lens patients.
“It reduces complications and increases the chances they will get the premium lens they paid for,” he said. “The capsulorhexis is geometrically perfect, which ensures centration. Small amounts of astigmatism can be treated, which helps ensure elimination of all refractive error.”
Dr. Williamson has used ORA intraoperative aberrometry (Alcon) for the past 5 years. He noted that it’s rare for him to have to change the spherical power, though he said he will routinely change the power of a toric lens.
Dr. Nikpoor said that she uses the LenSx laser (Alcon) with VERION (Alcon) in surgery. This can also help with marking the cornea and planning her axis.
She uses ORA for every premium case. “When I’m implanting a lens, if toric, I’ll use VERION and ORA axis alignment with my own marks,” she said, adding that she’ll use all three and see where the lens needs to go. She also uses the VERION system for centration of any presbyopia-correcting IOL, adding that she’s been using it to center the Light Adjustable Lens (RxSight) and Vivity (Alcon) as well.
She noted that her practice also has Callisto eye (Carl Zeiss Meditec), which she uses infrequently, and OPMI Lumera (Carl Zeiss Meditec), which can help center the lens.
Postop tools
Dr. Williamson said postop enhancements in his practice are done infrequently. If he does have to enhance, he will use iDesign (Johnson & Johnson Vision), as well as an aberrometer and OPD-Scan III (Nidek).
“The YAG laser is your friend with premium lens patients,” Dr. Walter said of postop interventions. “I think too often we shy away from the YAG treatment for fear that it might not help and will make the IOL exchange more difficult.” Dr. Walter has found that if the patient tolerated the typical dysphotopsias initially but then had more or reduced reading vision, a YAG capsulotomy can turn them into a happy patient.
Dr. Nikpoor’s practice uses the Alcon WaveLight Refractive Suite for enhancements. She said it’s important to make sure any ocular surface disease is under control and refraction is stable before proceeding with laser vision correction. She finds the PanOptix (Alcon) to be more sensitive to any PCO or residual refractive error than prior lenses, so she has a low threshold to YAG and enhance if it is going to benefit the patient.
ARTICLE SIDEBAR
Enhancement rates
When discussing technology to improve premium lens outcomes, the topic of postop enhancement came up among the members of the EyeWorld Refractive Editorial Board. Lance Kugler, MD, said that for patients undergoing refractive cataract surgery with multifocal IOLs and astigmatism management, the enhancement rate should be no lower than 10–12%, which sparked a discussion among board members about how often they perform enhancements.
Dr. Kugler noted that it’s difficult to compare enhancement rates among surgeons due to the inherently subjective nature of enhancements. “However, if one approaches multifocal IOLs with the assumption that anything more than 0.5 D of cylinder is unacceptable, the math suggests that an enhancement rate in the 10–12% range is required,” he said, adding that this is derived from the limitations of formulas, keratometry, axial length, effective lens position, and IOL manufacturing tolerances. A 20 D IOL may actually be significantly higher or lower power, Dr. Kugler said.
He added that those who perform more RLE than refractive cataract surgery are likely going to have a higher enhancement rate than those who do predominantly cataract surgery. Additionally, Dr. Kugler said that comanaged patients are likely to have a lower enhancement rate, as they may be offered enhancement less frequently.
Dr. Kugler noted that an informal survey among surgeons in the Refractive Surgery Alliance several years ago found the enhancement rate was 10–12%. “Anything less than that means a significant portion of patients out there are not seeing as well as they could be,” he said.
Dr. Kugler also noted the importance of having an enhancement plan in the event that one is needed and setting patient expectations prior to premium IOL surgery.
Thomas Clinch, MD, thinks the variation in surgeon enhancement rates may be attributable to setting appropriate patient expectations. He practices in Washington, D.C., and said it is a very demanding market with analytical, educated patients. Dr. Clinch’s enhancement rate is low (less than 2%). “This may be based on not performing a substantial amount of RLE and recommending that cataract patients defer surgery until they are truly symptomatic,” he said. “Part of that strategy is that at the time of surgery, they have reasonable expectations rather than expecting perfection. They are usually grateful for a good outcome.” He usually has patients wait 2–3 months before enhancing to achieve refractive and neuroadaptive stability, but he noted that in instances where a toric IOL rotates or there is a substantial refractive “surprise,” one needs to be proactive.
While performing a substantial surgical volume, Dr. Clinch’s practice pattern is not aggressive. He tends to allow patients to evolve toward the decision. “Building a community reputation of being a cautious but confident surgeon has been very rewarding. It has allowed me to build a large referral base of surrounding physicians and optometrists,” Dr. Clinch said.
John Berdahl, MD, said his enhancement rates for premium IOLs is about 10%.
Roger Zaldivar, MD, thinks enhancement rate depends on the prior state of your patients. “If you are doing RLE, you should be around 10% enhancement rate due to power estimations and astigmatism,” he said. “You can minimize this with lot of chair time.” It will depend on how aggressive you are at selling the procedure, too, Dr. Zaldivar said. “With new EDOF IOLs, since they have a larger landing zone, our enhancement rate is around 5%.”
Dr. Williamson has a low enhancement rate, noting that he tries to “treat the patients and not the numbers.” “We should remember that PRK and LASIK aren’t totally benign; they are still another surgery with their own set of issues and recovery. While I’m happy to use these technologies for unhappy patients and we include this in our refractive package, I’m not going to recommend it on happy patients simply because they have small amounts of residual refractive error,” he said.
Contact
Berdahl: john.berdahl@vancethompsonvision.com
Clinch: tclinch@edow.com
Kugler: lkugler@kuglervision.com
Williamson: blakewilliamson@weceye.com
Zaldivar: zaldivarroger@gmail.com
About the physicians
Neda Nikpoor, MD
Aloha Laser Vision
Honolulu, Hawaii
Keith Walter, MD
Wake Forest Baptist Health
Winston-Salem, North Carolina
Blake Williamson, MD
Williamson Eye Center
Baton Rouge, Louisiana
Relevant disclosures
Nikpoor: None
Walter: Johnson & Johnson Vision
Williamson: Johnson & Johnson Vision
Contact
Nikpoor: nnikpoor1@gmail.com
Walter: kwalter@wakehealth.edu
Williamson: blakewilliamson@weceye.com